杨延梦 张烽 唐艳隆 毕孝杨
【摘要】目的 探讨Zinner综合征的诊治要点,降低误诊率。方法 回顾性分析1例Zinner综合征患者的临床资料。以Zinner综合征、肾缺如以及精囊囊肿作为检索词,对以下数据库截至2022年11月收录的文献进行检索:PubMed、CNKI、万方数据知识服务平台、维普中文科技期刊数据库,收集并分析检索到的以血尿、尿频、尿痛等泌尿系统症状为首发表现的Zinner综合征病例,总结其临床特征、发育特点、治疗方法等。结果 该例患者为46岁男性,因发现膀胱占位性病变8年、出现血尿伴尿痛1周入院,经影像学检查确诊为Zinner综合征。接受经尿道膀胱镜检术+经直肠精囊囊肿抽吸术治疗,术程顺利,于术后第2日出院,遵医嘱于院外继续接受抗感染治疗。检索文献,共收集到16例以血尿、尿痛等泌尿系统症状为首发表现的Zinner综合征病例,均通过影像学检查发现泌尿系统异常,主要治疗方法是手术切除囊肿、囊肿穿刺抽吸等。接受了随访的8例患者中7例未见复发、1例接受精囊囊肿穿刺抽吸治疗的患者疑似复发。结论 Zinner综合征主要影像学表现为单侧精囊囊肿、同侧肾缺如和同侧射精管阻塞,超声检查、CT、MRI均是诊断Zinner综合征的重要手段,实施手术切除不易复发。
【关键词】Zinner综合征;精囊囊肿;肾缺如;残余输尿管;泌尿系统
Zinner syndrome: a case report and literature review
YANG Yanmeng, ZHANG Feng, TANG Yanlong , BI Xiaoyang
( Department of Radiology, the First Affiliated Hosptial of Dali University, Dali 671000, China)
Corresponding author: TANG Yanlong, E-mail: 754763105@qq.com
【Abstract】Objective To investigate the key issues of clinical diagnosis and treatment of Zinner syndrome and reduce the misdiagnosis rate. Methods Clinical data of 1 case of Zinner syndrome were retrospectively analyzed. Zinner syndrome cases presenting hematuria, frequent urination and dysuria as initial manifestations were retrieved from PubMed, CNKI, Wanfang Data and Chongqing VIP until November 2022 by using the searching words of Zinner syndrome, renal agenesis and seminal vesicle cyst. Clinical characteristics, developmental characteristics and treatment methods were summarized. Results The 46-year-old male patient was admitted to the hospital because of “bladder space-occupying lesion for more than 8 years, hematuria with dysuria for 1 week”, and was diagnosed with Zinner syndrome by imaging examination. He successfully underwent “transurethral cystoscopy + transrectal pelvic mass puncture biopsy”, and was discharged from the hospital at postoperative 2 d. The patient was advised to continually receive anti-infection treatment after discharge. According to literature review, 16 cases of Zinner syndrome presenting with hematuria, dysuria and other urinary symptoms as the first manifestations were collected. All patients developed abnormalities in the urinary system by imaging examination. Surgical resection and puncture biopsy were the main treatment methods. Among 8 patients receiving follow-up, 7 cases did not recur, and 1 suspected recurrent case underwent puncture biopsy. Conclusions Zinner syndrome is mainly manifested with imaging characteristics of unilateral seminal vesicle cyst, ipsilateral renal agenesis and ipsilateral ejaculatory duct obstruction triad. Ultrasound, CT scan, and MRI are important diagnostic tools for Zinner syndrome. Laparoscopic seminal vesicle cystectomy can reduce the risk of recurrence.
【Key words】Zinner syndrome; Seminal vesicle cyst; Renal agenesis; Residual ureter;Urinary system
Zinner综合征是一种罕见的先天性泌尿生殖系统发育异常性疾病,主要表现为单侧精囊囊肿、同侧肾缺如和同侧射精管阻塞三联征。多数Zinner综合征患者无明显症状,常在体检时才发现患有本病,当精囊囊肿直径超过5 cm时[1-2],患者多伴有尿频、尿痛、会阴部不适和射精后疼痛等非特异性症状[3]。现报告我院收治的1例Zinner综合征患者,并结合文献进行复习以提高临床医师对该病的诊治水平。
1 对象与方法
1.1 1例Zinner综合征患者临床资料的收集
回顾性分析我院2022年收治的1例Zinner综合征患者的临床资料。本研究获我院医学伦理委员会批准(批件号:DFY20221010001),患者对研究知情同意。
1.2 文献检索
以Zinner综合征(Zinner syndrome)、肾缺如(absence of kidney)以及精囊囊肿(seminal vesicle)为检索词,对以下数据库截至2022年11月收录的文献进行检索:PubMed、CNKI、万方数据知识服务平台、维普中文科技期刊数据库,收集并分析检索到的以血尿、尿频、尿痛等泌尿系统症状为首发表现的Zinner综合征病例,总结其临床特征、发病特点、治疗方法等。
2 结 果
2.1 1例Zinner综合征患者的临床资料
2.1.1 主诉及相关检查
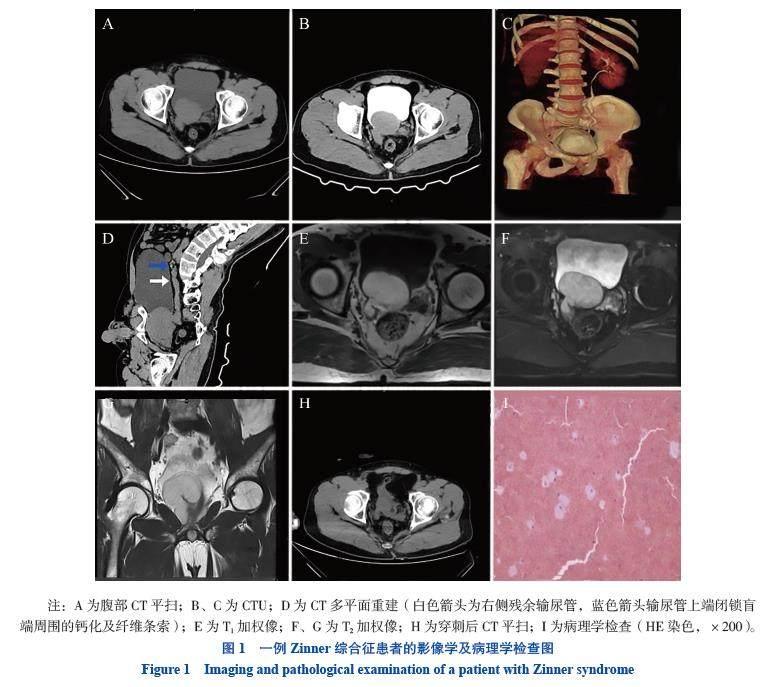
患者男,46岁,已婚已育。因发现膀胱占位性病变8年、出现血尿伴尿痛1周于2022年10月26日来我院就诊。患者于2014年10月12日进行体检,通过中下腹部CT平扫+增强扫描发现右肾缺如、左肾体积增大,且膀胱后壁有一大小约5.0 cm×3.0 cm的软组织密度影(图1A)。2015年4月1日再次复查中下腹部CT平扫,膀胱占位性病变无明显变化。本次入院1周前患者出现全程肉眼血尿伴尿痛,无明显诱因。2 d前患者再次出现上述症状,在当地县人民医院就诊,泌尿系统彩色多普勒超声检查(彩超)显示右肾缺如声像,膀胱无回声区声像;腹部CT平扫显示右肾缺如、膀胱占位性病变。
体格检查无明显异常。血尿粪常规、凝血功能、肿瘤全套检查(甲胎蛋白、癌胚抗原、血清铁蛋白、糖类抗原125、糖类抗原19-9、糖类抗原153、糖类抗原242、鳞状上皮细胞癌抗原、神经元特异性烯醇化酶、前列腺特异性抗原等)、肝功能检查、肾功能检查、凝血功能检查、传染性疾病检查、心电图、中段尿细菌培养等均未见异常。泌尿系统CT成像(CTU)显示右肾缺如,右侧残余输尿管近端向上延伸为闭锁的盲端,远端开口于精囊囊肿;左侧肾盂、肾盏、输尿管及膀胱内可见造影剂充盈;膀胱后方可见不规则团块影,性质待查(图1B~D)。彩超显示尿潴留声像。MRI平扫+增强扫描显示膀胱后方偏右侧存在不规则囊袋状改变(图1E~G)。患者最终被确诊患Zinner综合征。
2.1.2 治疗方法
患者经保守治疗无效,遂接受经尿道膀胱镜检术+经直肠盆腔肿块抽吸术治疗。在B超引导下,采用经皮肾穿刺针经直肠对患者盆腔内精囊囊肿进行穿刺,引出40 mL暗红色液体。观察穿刺部位无活动性出血,其后留置22F三腔尿管并结束手术。患者术后生命体征平稳,继续予其抗感染、营养补液等对症支持治疗。
2.1.3 转 归
术后第1日,复查中下腹部CT平扫,显示患者的膀胱占位性病变体积较术前明显缩小(图1H)。术后回报病理学检查结果为盆腔肿物内穿刺液血性背景,有效细胞较少,未检出肿瘤细胞(图1I)。术后第2日,患者生命体征平稳,未见明显异常表现,于当日出院,遵医嘱于院外继续接受抗感染治疗。随访至2024年1月,患者情况良好,未见复发。
2.2 文献检索结果
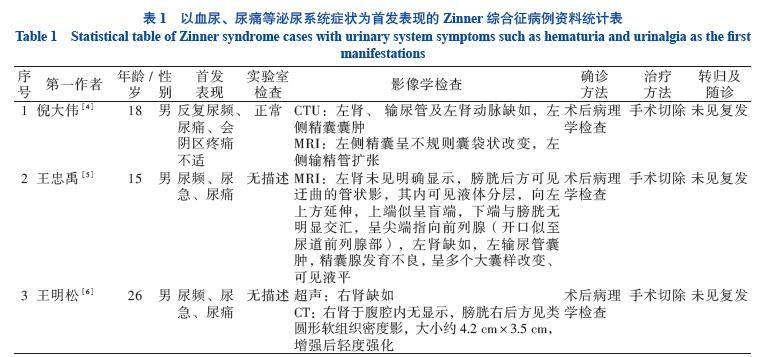
检索文献,共收集到16例以血尿、尿频、尿痛等泌尿系统症状为首发表现的Zinner综合征病例,均通过影像学检查发现泌尿系统异常,主要治疗方法是手术治疗、囊肿穿刺抽吸等。接受了随访的8例患者中7例未见复发、1例疑似复发。见表1。
3 讨 论
Zinner综合征多见于20~40岁处于性生活高峰年龄段的男性,主要表现为单侧精囊囊肿、同侧肾缺如和同侧射精管阻塞三联征,最先由Zinner于1914年报道[20],发病率约为2.14/100 000[1]。该病起源于肾导管,是泌尿生殖道胚胎发育不良所致。中肾管或Wolffian管是形成男性生殖系统以及输尿管芽的成对结构。在胚胎发育期间,输尿管芽分泌生长因子并增殖,与后肾母细胞融合,肾母细胞经诱导后由间充质向上皮转化进而形成原始肾脏,在诱导过程中出现任何一种干扰都会导致肾发育不全。同时,输尿管芽与中肾管下部分离失败,会导致射精管闭锁和精囊阻塞,使分泌物积聚,出现囊性扩张[21]。因此,Zinner综合征的主要表现是单侧射精管阻塞、同侧精囊囊肿和同侧肾发育不全。输尿管芽发育异常还可出现发育性锥体异常及形成重复的输尿管,例如四叉输尿管[12]。
超声检查通常是诊断Zinner综合征的首选方法,有较高的准确性和特异性。CT和MRI均可以准确定位精囊囊肿,而且两者的扫描范围大、视野广,常可同时发现其他器官的异常。MRI能准确显示男性生殖系统解剖结构[22],是最常用于诊断精囊囊肿的方法[23-24]。MRI能显示囊性病变与精囊之间的关系,可确定囊肿的起源,有助于鉴别精囊囊肿、输尿管囊肿和射精管囊肿。输尿管囊肿的CT和MRI常表现为类圆形囊样灶,边界清晰,密度均匀,可并发结石,也可并发同侧肾及输尿管积水,而无同侧肾缺如。射精管囊肿的MRI表现为T1加权像等信号或低信号,T2加权像高信号,对周围邻近器官无挤压,一般不伴有肾及输尿管的发育异常[25]。
关于Zinner综合征的治疗,若患者无症状或症状轻微,可行保守治疗,定期观察;当患者精囊囊肿较大且出现明显临床症状时,可经尿道、直肠对囊肿进行穿刺引流,也可进行开放手术或微创手术治疗[22]。其中腹腔镜手术已成为治疗Zinner综合征精囊囊肿的主要手段之一[26],特别是近年出现的机器人辅助腹腔镜手术[27]。Zinner综合征是罕见病,缺乏大样本多中心的研究,因此目前对于Zinner综合征精囊囊肿的最佳治疗方法尚未达成共识,仍有待收集更多的病例并对其治疗方法进行更深入的研究,才能提供更为详尽的可参考数据[22]。在本研究中,我院收治的Zinner综合征患者因担心出现术后并发症而拒绝接受手术切除治疗,在经直肠精囊囊肿抽吸术治疗后,患者恢复良好,但该治疗方法有复发风险,需嘱患者定期随访。
参 考 文 献
[1] FIASCHETTI V, GRECO L, GIURICIN V, et al. Zinner syndrome diagnosed by magnetic resonance imaging and computed tomography: role of imaging to identify and evaluate the uncommon variation in development of the male genital tract[J]. Radiol Case Rep, 2017, 12(1): 54-58. DOI: 10.1016/j.radcr.2016.10.007.
[2] TAN Z, LI B, ZHANG L, et al. Classifying seminal vesicle cysts in the diagnosis and treatment of Zinner syndrome: a report of six cases and review of available literature[J]. Andrologia, 2020, 52(1): e13397. DOI: 10.1111/and.13397.
[3] CITO G, SFORZA S, GEMMA L, et al. Infertility case presentation in Zinner syndrome: can a long-lasting seminal tract obstruction cause secretory testicular injury[J]. Andrologia, 2019, 51(11): e13436. DOI: 10.1111/and.13436.
[4] 倪大伟, 魏灿, 齐伟, 等. Zinner综合征一例报告并文献复习[J]. 中华腔镜泌尿外科杂志(电子版), 2022, 16(2): 173-176. DOI: 10.3877/cma.j.issn.1674-3253.2022.02.017.
NI D W, WEI C, QI W, et al. Zinner syndrome: a case report and literatures review[J]. Chin J Endourol Electron Ed, 2022, 16(2): 173-176. DOI: 10.3877/cma.j.issn.1674-3253.2022.02.017.
[5] 王忠禹, 鞠文, 李志勤, 等. Zinner综合征临床新诊疗1例[J]. 临床泌尿外科杂志, 2018, 33(5): 420-422. DOI: 10.13201/j.issn.1001-1420.2018.05.022.
WANG Z Y, JU W, LI Z Q, et al. A case of new clinical diagnosis and treatment of Zinner syndrome[J]. J Clin Urol, 2018, 33(5): 420-422. DOI: 10.13201/j.issn.1001-1420.2018.05.022.
[6] 王明松, 李波军, 刘旭东, 等. Zinner综合征的诊断和微创治疗(附2例报告并文献复习)[J]. 临床泌尿外科杂志, 2015, 30(12): 1118-1121. DOI: 10.13201/j.issn.1001-
1420.2015.12.017.
WANG M S, LI B J, LIU X D, et al. Diagnosis and minimally invasive treatment of Zinner syndrome(Report of two cases and literature review)[J]. J Clin Urol, 2015, 30(12): 1118-1121. DOI: 10.13201/j.issn.1001-1420.2015.12.017.
[7] 曹家栋, 朱首伦, 白遵光, 等. Zinner综合征1例报道并文献复习[J]. 中华男科学杂志, 2017, 23(5): 452-454. DOI: 10.13263/j.cnki.nja.2017.05.013.
CAO J D, ZHU S L, BAI Z G, et al. Zinner syndrome: a case report and review of the literature[J]. Natl J Androl, 2017, 23(5): 452-454. DOI: 10.13263/j.cnki.nja.2017.05.013.
[8] 廖阳英, 潘少恒, 刘光德, 等. Zinner综合征1例[J]. 医学影像学杂志, 2021, 7(12):2155-2156.
LIAO Y Y, PAN S H, LIU G D, et al. Ultrasound diagnosis and treatment of zinner syndrome: one case report[J]. J Med Imag, 2021, 7(12):2155-2156.
[9] RAHOUI M, OUANES Y, CHAKER K, et al. An unusual cause of painful ejaculation in a young patient: Zinner syndrome[J]. Ann Med Surg, 2022, 79: 103982. DOI: 10.1016/j.amsu.2022.103982.
[10] GURUNG B, PANTA O B, DHAKAL V, et al. Zinner syndrome: a case report of rare urogenital anomaly[J]. J Med Ultrasound, 2022, 30(1): 59-61. DOI: 10.4103/JMU.JMU_125_20.
[11] GORANTLA R, ALLU S, RAO A. A triad of unilateral renal dysgenesis with ipsilateral seminal vesical and ejaculatory duct obstruction: an uncommon urogenital congenital anomaly, zinner syndrome-a case report[J]. Indian J Radiol Imaging, 2021, 31(3): 707-709. DOI: 10.1055/s-0041-1735503.
[12] FOLADI N, NASERY M N. Right-sided Zinner syndrome with a left side quadrupled ureter- a case report[J]. Radiol Case Rep, 2021, 16(10): 2873-2877. DOI: 10.1016/j.radcr.2021.06.086.
[13] ALARIFI M, AL-GAHWARY M, GOMHA M. The association of renal agenesis and ipsilateral seminal vesicle cyst: zinner syndrome case report[J]. Case Rep Urol, 2019, 2019: 1242149. DOI: 10.1155/2019/1242149.
[14] NAVAL-BAUDIN P, CARRE?O GARC?A E, SANCHEZ MARQUEZ A, et al. Multicystic seminal vesicle with ipsilateral renal agenesis: two cases of Zinner syndrome[J]. Scand J Urol, 2017, 51(1): 81-84. DOI: 10.1080/21681805.2016.1257650.
[15] SLAOUI A, REGRAGUI S, LASRI A, et al. Zinners syndrome: report of two cases and review of the literature[J]. Basic Clin Androl, 2016, 26: 10. DOI: 10.1186/s12610-016-0037-4.
[16] KARDOUST PARIZI M, SHAKHSSALIM N. Management of zinners syndrome associated with contralateral seminal vesicle hypoplasia: a case report[J]. Case Rep Urol, 2013, 2013: 494215. DOI: 10.1155/2013/494215.
[17] PEREIRA B J, SOUSA L, AZINHAIS P, et al. Zinners syndrome: an up-to-date review of the literature based on a clinical case[J]. Andrologia, 2009, 41(5): 322-330. DOI: 10.1111/j.1439-0272.2009.00939.x.
[18] MILITARU V, MIHALY Z A, ILEA C, et al. Zinner syndrome-
case report[J]. Med Pharm Rep, 2021, 94(Suppl No 1): S47-S50. DOI: 10.15386/mpr-2229.
[19] JUHO Y C, WU S T, TANG S H, et al. An unexpected clinical feature of zinners syndrome-A case report[J]. Urol Case Rep, 2015, 3(5): 149-151. DOI: 10.1016/j.eucr.2015.06.015.
[20] AUA PRACTICE GUIDELINES COMMITTEE. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations[J]. J Urol, 2003, 170(2 Pt 1): 530-547. DOI: 10.1097/01.ju.0000078083.38675.79.
[21] MEHRA S, RANJAN R, GARGA U C. Zinner syndrome-a rare developmental anomaly of the mesonephric duct diagnosed on magnetic resonance imaging[J]. Radiol Case Rep, 2016, 11(4): 313-317. DOI: 10.1016/j.radcr.2016.04.002.
[22] OSTROWSKA M, GRZE?K M, KACZY?SKI S, et al. Zinner syndrome-a rare cause of recurrent epididymitis and infertility[J]. Clin Pract, 2021, 11(4): 942-946. DOI: 10.3390/clinpract11040108.
[23] LIU T, LI X, HUANG L, et al. Zinner syndrome: an updated pooled analysis based on 214 cases from 1999 to 2020: systematic review[J]. Ann Palliat Med, 2021, 10(2): 2271-2282. DOI: 10.21037/apm-20-1997.
[24] 吴志平, 赵晓昆, 钟朝晖, 等. 输尿管异位开口合并肾发育畸形3例并文献复习[J]. 新医学, 2009, 40(3): 168-170. DOI: 10.3969/j.issn.0253-9802.2009.03.011.
WU Z P, ZHAO X K, ZHONG (C /Z)H, et al. Ectopic ureteral orifice complicated with renal developmental malformation: 3 cases report and literature review[J]. J New Med, 2009, 40(3): 168-170. DOI: 10.3969/j.issn.0253-9802.2009.03.011.
[25] 李英丽, 庄雄杰, 吴明哲, 等. Zinner综合征的CT和MRI表现[J]. 临床放射学杂志, 2021, 40(1): 101-105. DOI: 10.13437/j.cnki.jcr.2021.01.024.
LI Y L, ZHUANG X J, WU M Z, et al. CT and MRI findings of zinner syndrome[J]. J Clin Radiol, 2021, 40(1): 101-105. DOI: 10.13437/j.cnki.jcr.2021.01.024.
[26] ZHANG D X, LI X G, GAO Y, et al. Transperitoneal laparoscopic excision of seminal vesicle cyst: a single-center experience[J]. J Endourol, 2012, 26(9): 1153-1158. DOI: 10.1089/end.2012.0071.
[27] ALTOBELLI E, BOVE A, FALAVOLTI C, et al. Robotic-assisted laparoscopic approach in the treatment for Zinners Syndrome associated with ipsilateral megaureter and incomplete double-crossed ectopic ureter[J]. Int Urol Nephrol, 2013, 45: 635-638. DOI: 10.1007/s11255-013-0412-4.
(责任编辑:洪悦民)



