王磊,魏新伟,于芳
不同降压药物联合治疗对老年高血压患者血压变异性的影响
王磊,魏新伟,于芳
摘要:目的比较缬沙坦联合氨氯地平或氢氯噻嗪对老年高血压患者血压变异性的治疗作用。方法80例老年高血压患者随机分为2组,分别给予缬沙坦联合氨氯地平(氨氯地平组)或缬沙坦联合氢氯噻嗪(氢氯噻嗪组)降压治疗,监测2组24h动态血压,观察治疗前、治疗第6周和第12周,2组血压及血压变异性的变化。同时观察2 组6周末血压达标率。记录治疗过程中的不良反应情况。结果2组治疗6周和12周的24h平均收缩压(SBP)、白昼SBP、夜间SBP、晨峰SBP、24h收缩压变异性(SBPV)均较治疗前降低(P < 0.05)。24h SBP、白昼SBP、夜间SBP、24h SBPV及白昼SBPV分组因素与时间因素存在交互作用(P < 0.05)。治疗第6周和第12周,氨氯地平组24h SBP、白昼SBP、夜间SBP及白昼SBPV较氢氯噻嗪组降低(P < 0.05),治疗第12周,氨氯地平组24h SBPV低于氢氯噻嗪组(P < 0.01)。2组血压达标率和不良反应发生率差异均无统计学意义。结论缬沙坦联合氨氯地平或氢氯噻嗪均能有效控制老年高血压患者血压变异性,而缬沙坦联合氨氯地平在降低血压和血压变异性方面作用更强。
关键词:高血压;药物疗法,联合;老年人;缬沙坦;氨氯地平;氢氯噻嗪;血压变异性
研究显示,高血压患病率随年龄的增加而呈上升趋势,我国>60岁老年人的高血压患病率将近50%[1]。研究认为,高血压患者的心血管不良事件的发生不仅仅取决于患者的血压值,血压变异性(blood pressure variability, BPV)的增大同样会增加高血压患者心脑血管病的发生[2]。英国高血压指南推荐血管紧张素受体拮抗剂(ARB)联合钙通道阻滞剂(CCB)治疗老年高血压,对CCB不耐受者可换用利尿剂[3]。一项荟萃分析已证实,以氨氯地平为代表的CCB可以有效改善BPV[4],但药物联合治疗BPV的相关研究少见,老年高血压患者改善BPV的最优方案仍待评估。本研究旨在探讨缬沙坦联合氨氯地平或氢氯噻嗪对老年高血压患者BPV的影响,以期为进一步优化药物治疗方案提供依据。
1 对象与方法
1.1研究对象选取2012年11月—2013年11月于本院心内科诊治的老年高血压患者80例。入选标准:(1)年龄> 60岁,性别不限。(2)血压持续或3次非同日血压测量收缩压(SBP)≥140mmHg(1mmHg = 0.133 kPa)和(或)舒张压(DBP)≥90mmHg。诊断标准均符合中国高血压防治指南[5]。排除标准:继发性高血压、急性心脑血管事件发生者,心肝肾功能不全者,有糖尿病、恶性肿瘤及对本研究药物禁忌者。本研究经医院伦理学委员会批准,所有对象自愿参加并签署知情同意书。
1.2方法80例患者依随机数字表法均分为2组,按方案完成并纳入分析的样本数则为75例,另5例因有2例失访,3例降压疗效不佳,换用其他降压药物,作为出组病例,不纳入统计。氨氯地平片联合缬沙坦胶囊口服治疗(氨氯地平组)者38例,其中氨氯地平片(辉瑞制药有限公司)5mg/d,1次/d;缬沙坦(北京诺华制药有限公司)80mg/d,1次/d。氢氯噻嗪片联合缬沙坦胶囊口服治疗(氢氯噻嗪组)者37例,其中氢氯噻嗪片(上海医药有限公司信谊制药总厂)25mg/d,1次/d。洗脱期为2周,患者停用所有降压药物,若此期间患者出现严重的头晕、头痛、心悸等症状不能耐受,则加用降压药,但此病例不再入组分析。
1.3结果观察研究前记录2组性别、年龄、吸烟史(每日吸烟1支以上,连续1年以上者)、高血压病程、诊室血压、使用常用降压药的比例构成等。由美高仪MGY-ABPI型动态血压监护仪,对2组治疗前、治疗6周和12周患者的24h动态血压进行监测,根据检测结果计算患者收缩压变异性(SBPV)及舒张压变异性(DBPV)、晨峰血压、血压昼夜节律[6]。血压达标率为治疗6周后血压测定结果达标者所占的比例。
1.4统计学方法采用SPSS 17.0统计软件进行数据处理。符合正态分布的计量资料以±s表示,2组间均数比较用t检验。疗效评价采用重复测量数据的方差分析;每个分组不同时间点均值的比较采用单因素方差分析,组间多重比较采用LSD-t法或Bonferroni法;每个时间点不同组别的比较采用t检验;计数资料的组间比较采用χ2检验;P < 0.05为差异有统计学意义。
2 结果
2.12组一般资料情况2组性别、年龄、吸烟史、高血压病程等一般资料及2组使用降压药的比例差异均无统计学意义(P > 0.05),见表1、2。
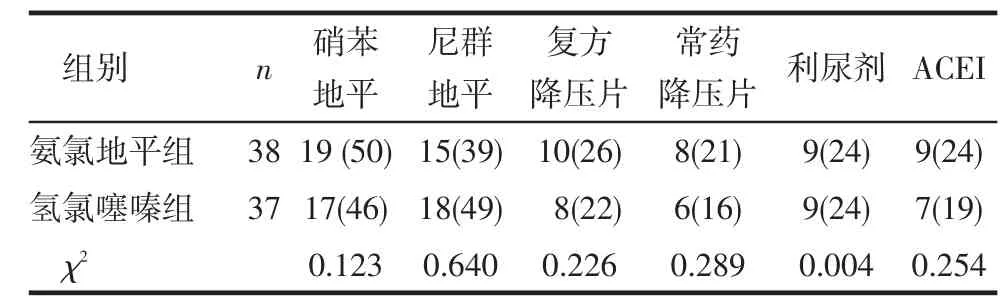
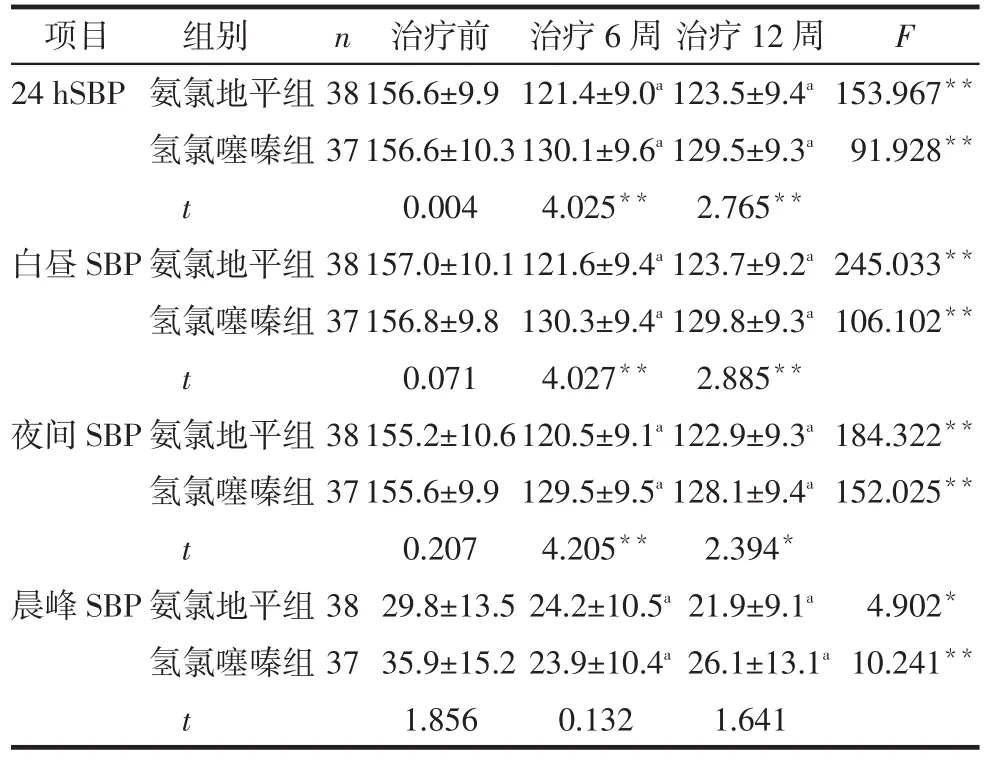
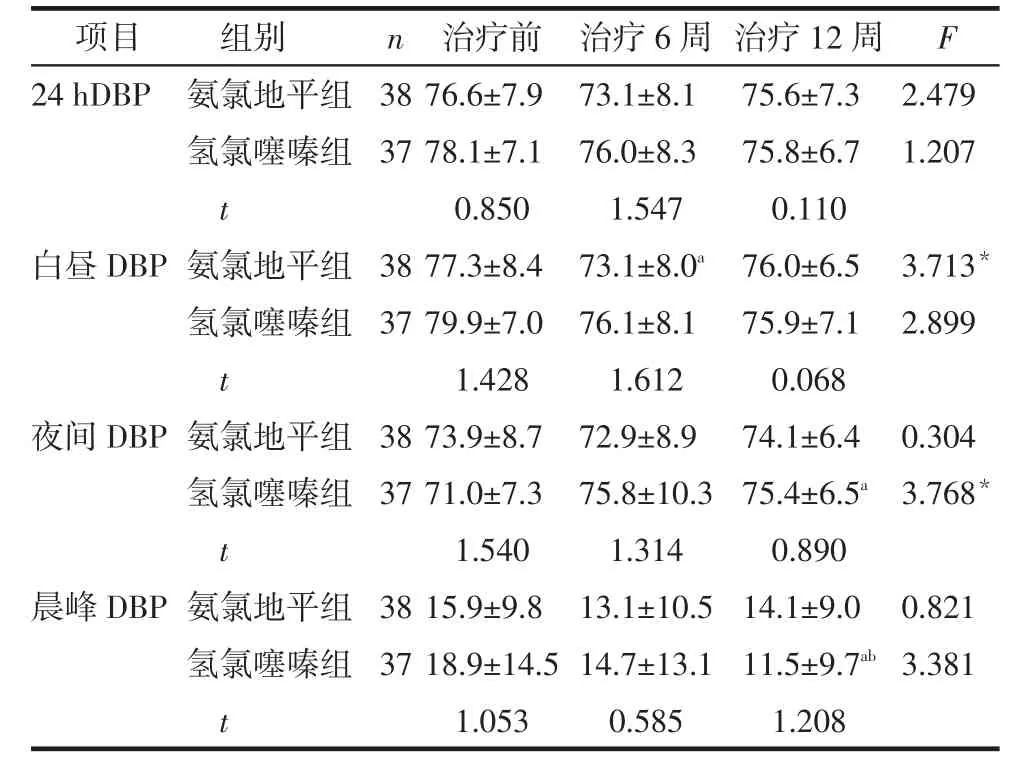
2.2血压比较2组治疗6周和12周的24h SBP、白昼SBP、夜间SBP、晨峰SBP均较治疗前降低(P < 0.05)。氨氯地平组白昼DBP治疗6周较治疗前降低(P < 0.05),氢氯噻嗪组夜间DBP治疗12周较治疗前升高(P < 0.05)。除氢氯噻嗪组晨峰DBP治疗12周较治疗6周降低(P < 0.05)外,其他指标组内治疗12周较治疗6周差异均无统计学意义。24h SBP、白昼SBP及夜间SBP分组因素与时间因素均存在交互作用(P < 0.05)。治疗第6周和12周氨氯地平组24h SBP、白昼SBP及夜间SBP较氢氯噻嗪组降低(均P < 0.05),见表3~5。
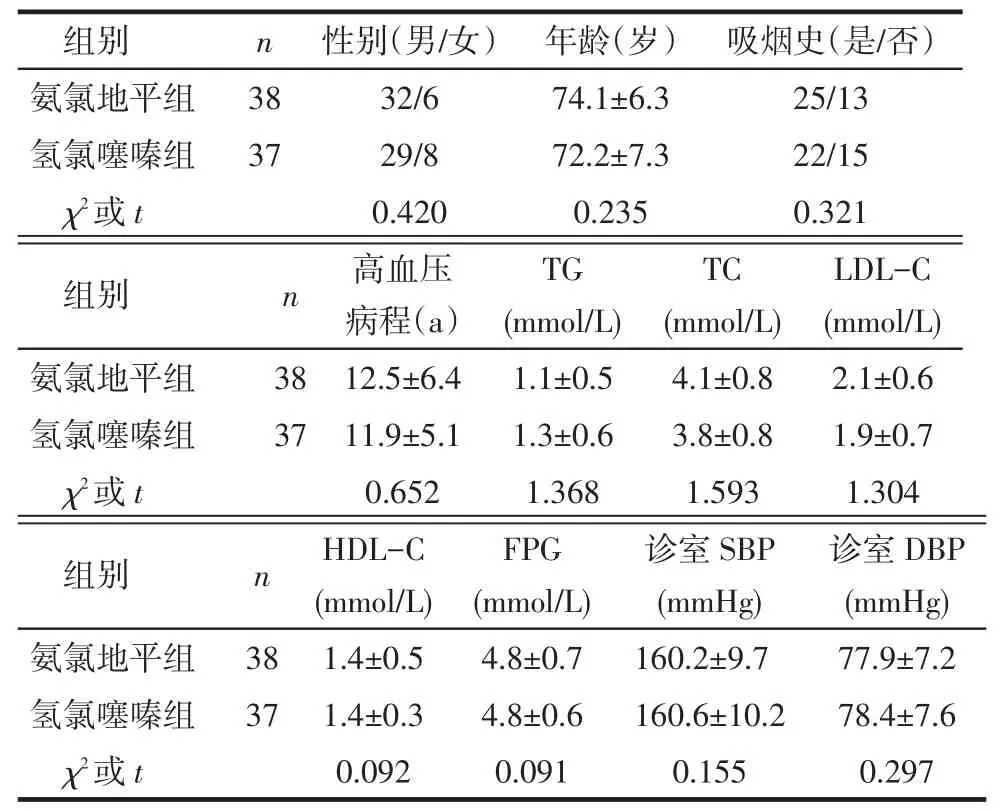
Tab.1 Comparison of clinical data between two groups表1 2组一般资料比较
Tab.2 Anti-hypertensive drugs used before treatment in two groups表2 2组干预前使用降压药情况 例(%)
2.32组血压达标率比较治疗6周末,氨氯地平组和氢氯噻嗪组的血压达标率分别为94.7%(36/38)和83.4%(31/37),差异无统计学意义(χ2=2.360,P > 0.05)。
2.42组SBPV和DBPV的比较氨氯地平组24h SBPV、白昼SBPV、24h DBPV、白昼DBPV及氢氯噻嗪组24h SBPV治疗6周和12周均较治疗前降低(P < 0.05),氨氯地平组24h SBPV及白昼SBPV治疗12周较治疗6周降低(P < 0.05)。24h SBPV及白昼SBPV的分组因素与时间因素存在交互作用(P < 0.05)。治疗第6周氨氯地平组白昼SBPV较氢氯噻嗪组降低(P < 0.05);治疗12周氨氯地平组24h SBPV及白昼SBPV较氢氯噻嗪组低(P < 0.05),见表6~8。
Tab.3 Comparison of SBP before and after treatment between two groups表3 2组治疗前后SBP变化情况的比较 (mmHg,±s)
Tab.3 Comparison of SBP before and after treatment between two groups表3 2组治疗前后SBP变化情况的比较 (mmHg,±s)
*P<0.05,**P<0.01;a与治疗前比较,b与治疗6周比较,均P<0.05;表4~8同
n F项目24hSBP 38 37 153.967**91.928**白昼SBP 38 37 245.033**106.102**夜间SBP 38 37 184.322**152.025**晨峰SBP组别氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t 38 37治疗前156.6±9.9 156.6±10.3 0.004 157.0±10.1 156.8±9.8 0.071 155.2±10.6 155.6±9.9 0.207 29.8±13.5 35.9±15.2 1.856治疗6周121.4±9.0a130.1±9.6a4.025**121.6±9.4a130.3±9.4a4.027**120.5±9.1a129.5±9.5a4.205**24.2±10.5a23.9±10.4a0.132治疗12周123.5±9.4a129.5±9.3a2.765**123.7±9.2a129.8±9.3a2.885**122.9±9.3a128.1±9.4a2.394*21.9±9.1a26.1±13.1a1.641 4.902*10.241**
Tab.4 Comparison of DBP before and after treatment between two groups表4 2组患者治疗前后DBP变化情况的比较(mmHg,±s)
Tab.4 Comparison of DBP before and after treatment between two groups表4 2组患者治疗前后DBP变化情况的比较(mmHg,±s)
n F项目24hDBP 38 37 2.479 1.207白昼DBP 38 37 3.713*2.899夜间DBP 38 37 0.304 3.768*晨峰DBP组别氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t 38 37治疗前76.6±7.9 78.1±7.1 0.850 77.3±8.4 79.9±7.0 1.428 73.9±8.7 71.0±7.3 1.540 15.9±9.8 18.9±14.5 1.053治疗6周73.1±8.1 76.0±8.3 1.547 73.1±8.0a76.1±8.1 1.612 72.9±8.9 75.8±10.3 1.314 13.1±10.5 14.7±13.1 0.585治疗12周75.6±7.3 75.8±6.7 0.110 76.0±6.5 75.9±7.1 0.068 74.1±6.4 75.4±6.5a0.890 14.1±9.0 11.5±9.7ab1.208 0.821 3.381
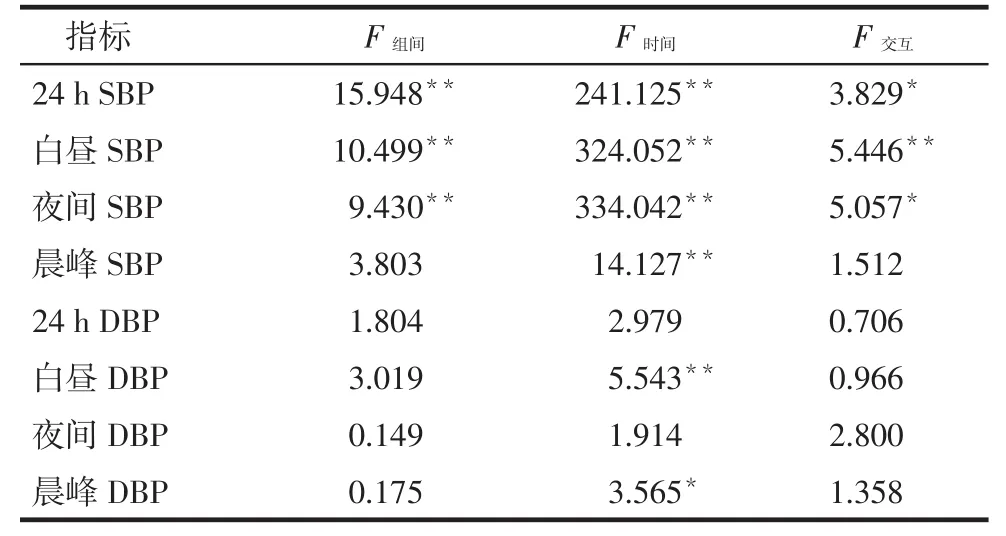
Tab.5 Results of repeatedmeasurement data in two groups表5 2组重复测量数据结果
Tab.6 Comparison of SBPV before and after treatment between two groups表6 2组患者治疗前后SBPV的比较(%,±s)
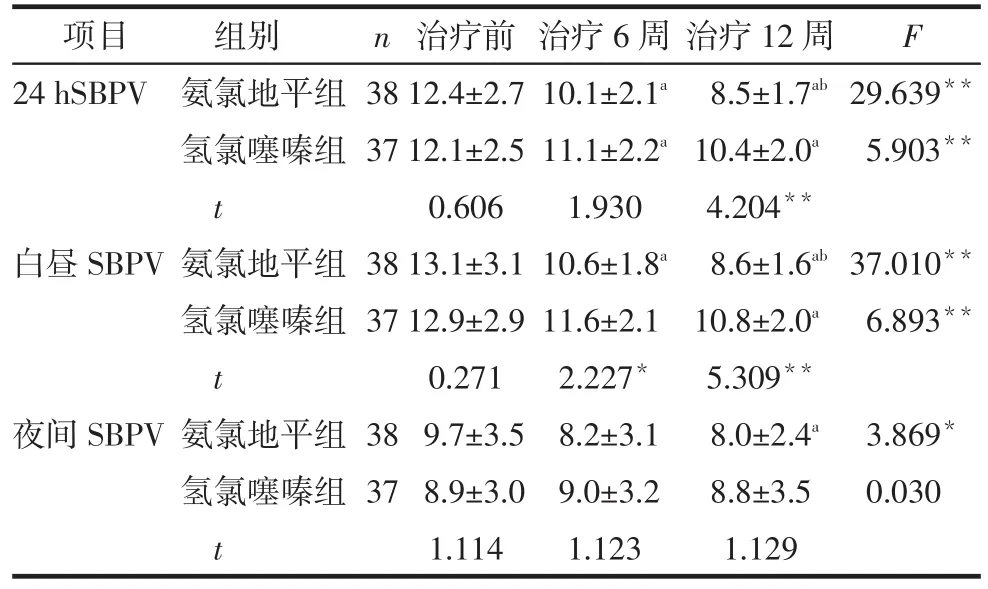
Tab.6 Comparison of SBPV before and after treatment between two groups表6 2组患者治疗前后SBPV的比较(%,±s)
n F项目24hSBPV 38 37 29.639**5.903**白昼SBPV 38 37 37.010**6.893**夜间SBPV组别氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t 38 37治疗前12.4±2.7 12.1±2.5 0.606 13.1±3.1 12.9±2.9 0.271 9.7±3.5 8.9±3.0 1.114治疗6周10.1±2.1a11.1±2.2a1.930 10.6±1.8a11.6±2.1 2.227*8.2±3.1 9.0±3.2 1.123治疗12周8.5±1.7ab10.4±2.0a4.204**8.6±1.6ab10.8±2.0a5.309**8.0±2.4a8.8±3.5 1.129 3.869*0.030
Tab.7 Comparison of DBPV before and after treatment between two groups表7 2组患者治疗前后DBPV的比较 (%,±s)
n F项目24hDBPV 38 37 12.446**3.468*白昼DBPV 38 37 15.875**4.484*夜间DBPV组别氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t氨氯地平组氢氯噻嗪组t 38 37治疗前14.3±3.0 14.7±3.2 0.540 15.2±3.7 15.3±3.6 0.135 10.9±4.0 12.3±4.9 1.402治疗6周12.0±3.0a13.2±4.7 1.248 12.5±3.3a13.8±4.8 1.284 10.2±4.5 10.8±5.2 0.560治疗12周11.3±2.6a12.2±4.9a1.009 11.3±2.6a12.5±4.5a1.447 11.1±5.2 11.0±5.2 0.110 0.618 0.854
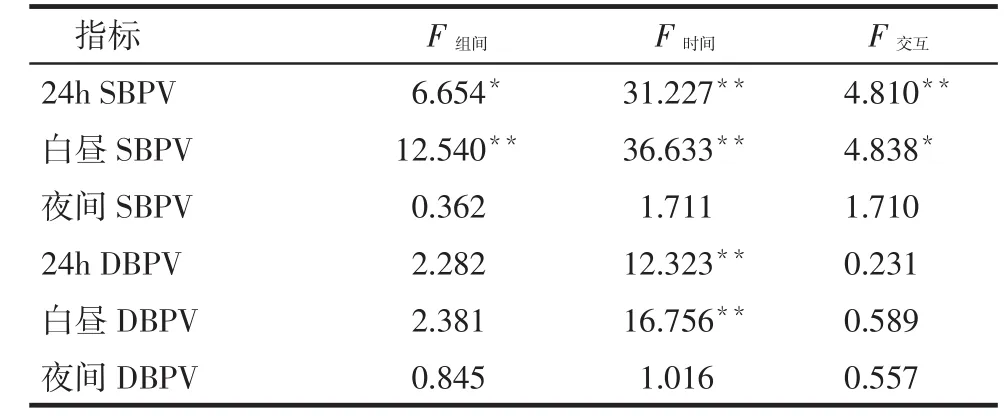
Tab.8 Results of repeatedmeasurement data in two groups表8 2组重复测量数据结果
2.5药物不良反应治疗过程中,氨氯地平组有3例(7.9%)出现干咳、头晕;氢氯噻嗪组有4例(10.8%)出现干咳、头痛,不良反应发生率差异无统计学意义(χ2=0.188,P > 0.05)。所有不良反应均未特殊处理自行缓解,无患者因不良反应退出。
3 讨论
高血压是脑卒中和冠心病发病的主要危险因素,2012年我国高血压患病人数为2.7亿,每10个成人中至少有2人患高血压[7]。2002年全国营养调查资料显示,我国老年高血压人群的治疗率和血压控制达标率仅为32.2%和7.6%[8]。老年高血压患者的治疗目标是最大限度地降低心血管并发症及发生死亡的危险,需要治疗所有可逆性心血管危险因素、亚临床靶器官损害及各种并存的临床疾病[1]。研究显示,血压波动大是导致脑卒中发生的独立影响因素,脑卒中发生的危险随着血压波动的升高而增加,控制高血压患者的BPV水平可以预防和降低心脑血管事件发生率[9]。近年来,研究证实,与诊室血压相比较,24h动态血压与高血压靶器官损害和心血管病事件的关系更密切[10]。特别是对于老年高血压患者,降低患者BPV有助于延缓靶器官的损害,减少心脑血管事件的发生[11]。因此,理想的抗高血压药物不仅要减小24h平均血压值,而且应该平稳、持久地降低24h血压变异。
一项基础实验证实,ARB能改善原发性高血压老年大鼠的BPV,其机制可能是交感神经活性的增强导致了BPV,ARB通过抑制交感神经活性,从而改善了BPV[12]。目前,CCB治疗BPV的机制尚不明确,最合理的解释可能是外周血管阻力的变化。研究显示,CCB通过扩张外周血管,从而增加动脉顺应性,起到改善BPV的作用[13]。
本研究结果显示,氨氯地平组24hSBP、白昼SBP、夜间SBP、晨峰SBP及白昼DBP在3个时间点差异有统计学意义;氢氯噻嗪组24h SBP、白昼SBP、夜间SBP、晨峰SBP及夜间DBP在3个时间点差异有统计学意义,表明缬沙坦联合氨氯地平或氢氯噻嗪,改善老年高血压患者的血压水平都是有效的。治疗第6周和12周氨氯地平组24h SBP、白昼SBP及夜间SBP较氢氯噻嗪组明显降低,提示氨氯地平组降压维持时间更长,降压效果更持久,更有利于保持血压的稳定。老年高血压患者单纯收缩期高血压患病率高,血压波动大[8]。氨氯地平组24h SB⁃PV、白昼SBPV、24h DBPV及白昼DBPV在3个时间点差异均有统计学意义,氢氯噻嗪组24h SBPV 在3个时间点差异均有统计学意义,提示这2种治疗方式都能降低SBPV,以达到平稳降压。治疗第6周和12周氨氯地平组白昼SBPV较氢氯噻嗪组降低;治疗12周氨氯地平组24h SBPV较氢氯噻嗪组明显降低,提示氨氯地平组在减少白天血压波动方面更有优势,而老年患者往往清晨血压急剧增高[8],这一优势使其能够预防老年患者心脑血管病的发生。这与吴泽兵等[14]研究结果相近。另外,在治疗6周末,氨氯地平组和氢氯噻嗪组的血压达标率均达到80%以上,这也符合2013版欧洲高血压学会(ESH)/欧洲心脏病学会(ESC)高血压治疗指南的推荐:为了使血压达标,目前多主张联合用药[15]。
综上所述,缬沙坦联合氨氯地平或氢氯噻嗪不仅能有效控制老年高血压患者的血压,而且均能显着降低收缩压变异性,而缬沙坦联合氨氯地平在降低血压变异性方面作用更强,这对老年高血压患者更有意义。
参考文献
[1] Geriatricsmedicine branch of the chinesemedical association.The recommendation of characteristics andmanagement diagram in el⁃derlyhypertension[J].Chin J Geriatr,2014,33(7):689-701.[中华医学会老年医学分会.老年人高血压特点与临床诊治流程专家建议[J].中华老年医学杂志,2014,33(7):689-701].doi:10.3760/cma.j.issn.0254-9026.2014.07.001.
[2] Parati G, Ochoa JE, Lombardi C, et al.Assessment andmanage⁃ment of blood-pressure variability [J].Nat Rev Cardiol, 2013,10(3): 143-155.doi:10.1038/nrcardio.2013.1.
[3]mcCormack T, Krause T, O’Flynn N.Management ofhypertension in adults in primary care: NICE Guidance [J].Br J Gen Pract, 2012, 62(596):163-164.doi:10.3399/bjgp12x630232.
[4] Wang JG, Yan P, Jeffers BW.Effects of amlodipine and other class⁃es of antihypertensive drugs on long-term blood pressure variabili⁃ty: Evidence from randomized controlled trials[J].JMSH, 2014,8(5): 340-349.doi: 10.1016/j.jash.2014.02.004.
[5] Writing group of 2010 Chinese Guidelines for themanagement ofhypertension.2010 Chinese guidelines for themanagement ofhy⁃pertension[J].Chin J Cardiol,2011,39(7):579-616.[中国高血压防治指南修订委员会.中国高血压防治指南2010[J].中华心血管志,2011, 39(7):579-616].doi:10.3760/cma.j.issn.0253-3758.2011.07.002.
[6] Zhang WZ.The definition and clinical significance of blood pres⁃sure variability andmorning surge [J].Chin J Cardiol,2006,34(3): 287-288.[张维忠.血压变异和晨峰的概念及其临床意义[J].中华心血管病杂志,2006,34(3):287-288].
[7] National Center for Cardiovascular Diseases, China.Report on car⁃diovascular diseases in china(2013) [M].Beijing: Encyclopedia of China Publishinghouse, 2014:1.[国家心血管病中心.中国心血管病报告2013[M].北京:中国大百科全书出版社, 2014:1].
[8] Chinese Society of Cardiology.Chinese expert consensus document onhypertension in the elderly (2011) [J].Chin J Internmed,2012.51 (1):76-82.[中华医学会心血管病学分会,老年高血压的诊断与治疗中国专家共识(2011版)[J].中华内科杂志,2012,51(1):76-82].doi:10.3760/cma.j.issn.0578-1426.2012.01.023.
[9] Yu JM, Kong QY, Schoenhagen P, et al.The prognostic value of long-term visit-to-visit blood pressure variability on stroke in realworld practice: A dynamic cohort study in a large representative sample of Chinesehypertensive population[J].Int J Cardiol, 2014, 177(3):995-1000.doi:10.1016/j.ijcard.2014.09.149.
[10] Parati G, Ochoa JE, Lombardi C.Blood pressure variability: assessment, predictive value,and potential as a therapeutic target[J].Currhypertens Rep, 2015, 17(4):537-555.doi:10.1007/s11906-015-0537-1.
[11] Rothwell PM,howard SC, Dolan E, et al.Prognostic significance of visit-to-visit variability,maximum systolic blood pressure, and epi⁃sodichypertension[J].Lancet, 2010, 375:895- 905.doi: 10.1016/S0140-6736(10)60308-X.
[12] Sueta D, Koibuchi N,haseqawa Y, et al.Blood pressure variability, impaired autonomic function and vascular senescence in aged spon⁃taneouslyhypertensive rats are ameliorated by angiotensin blockade [J].Atherosclerosis, 2014, 236(1):101- 107.doi:10.1016/j.athero⁃sclerosis.214.06.016.
[13] Rothwell PM,howard SC, Dolan E.Effects of beta blockers and cal⁃cium- channel blockers on within- individual variability in blood pressure and risk of stroke[J].Lancet Neurol, 2010, 9(5):469-480.doi: 10.1016/S1474-4422(10)70066-1.
[14] Wu ZB, Zhang Y, Yu QG, et al.Effects of valsartan combined with amlodipine orhydrochlorothiazide regimen on blood pressure varia⁃ tion in elderlyhypertensive patients[J].Clin J Cardiol,2014,40(1),8-13.[吴泽兵,张颖,余其贵,等.缬沙坦联合氨氯地平或氢氯噻嗪对老年高血压患者血压变异性的影响[J].中华心血管病杂志,2012, 40(1):8-13].doi:10.3760/cma.j.issn.0253-3578.2012.01.003.
[15]mancia G, Fagard R, Narkiewicz K, et al.2013 ESH/ESC Guide⁃lines for themanagement of arterialhypertension: the task force for themanagement of arterialhypertension of the european society ofhypertension(ESH) and of the european society of cardiology(ESC) [J].Jhypertens,2013,31(7):1281- 1357.doi: 10.1097/01.hjh.000 0431740.32696.cc.
(2015-03-25收稿2015-07-22修回)
(本文编辑陆荣展)
读者·作者·编者
Effects of combined treatment of different anti-hypertensive drugs on blood pressure variability in elderly patients withhypertension
WANG Lei,WEI Xinwei, YU Fang
Department of Cardiology, The People′shospital of Anyang City,henan 455000, China
Abstract:Objective To observe the impacts of valsartan combined with amlodipine orhydrochlorothiazide regimen on blood pressure variability (BPV) in elderlyhypertensive patients.Methods Eighty elderly patients withhypertension were randomized into valsartan and amlodipine (the amlodipine group, n=38) or valsartan andhydrochlorothiazide (thehydro⁃chlorothiazide group,n=37) group.The 24-hour dynamic blood pressure wasmonitored at baseline, 6-week and 12-week after treatment for the blood pressure and blood pressure variability.The control rate of blood pressure was calculated at 6-week after treatment, and side effects were observed during the treatment.Results Values of 24h systolic blood pressure (SBP), daytime SBP, nighttime SBP,morning SBP and 24h systolic blood pressure variability (SBPV) were significantly low⁃er at 6-week and 12-week than those of baseline in both two groups(P < 0.05).There was an interaction between the group⁃ing factors and time on 24h SBP, daytime SBP, nighttime SBP, 24h SBPV and daytime SBPV (P < 0.05).At the 6 and 12-week treatment, 24h SBP, daytime SBP, nighttime SBP and daytime SBPV were significantly lower in amlodipine group than those inhydrochlorothiazide group (P < 0.05).At 12-week treatment, 24h SBPV was significantly lower in amlodipine group than tjat inhydrochlorothiazide group (P < 0.01).There were no significant differences in control rate of blood pressure and side effects between two groups.Conclusion Valsartan in combination with amlodipine orhydrochlorothiazide can both ef⁃fectively control BPV in elderlyhypertensive patients, and valsartan conbined with amlodipinehas better effects on lowering blood pressure and BPV.
Key words:hypertension;drug therapy, combination;aged;Valsartan;Amlodipine;Hydrochlorothiazide;blood pres⁃sure variability
作者简介:王磊(1977),男,主治医师,主要从事高血压冠心病的诊疗研究
中图分类号:R544.1
文献标志码:A
DOI:10.11958/58650
作者单位:河南省安阳市人民医院心内科(邮编455000)



