马魁 华英汇 李宏云 张健 陈世益
复旦大学附属华山医院运动医学科(上海 200040)
踝关节外侧副韧带定量解剖研究
马魁 华英汇 李宏云 张健 陈世益
复旦大学附属华山医院运动医学科(上海 200040)
目的:通过对人体踝关节标本的定量解剖,明确踝关节外侧副韧带相关形态参数及其起止点足印区至各解剖标志的距离,为踝关节外侧副韧带重建手术提供解剖学依据。方法:共选取19例下肢尸体标本,对踝关节外侧副韧带进行精细解剖观察并对相关参数如长度、宽度、厚度及其起止点至各解剖标志的距离进行定量测量。结果:19例人体下肢标本中,前距腓韧带(ATFL)平均长度为23.1±2.98 mm,其中单束8例(42.1%),双束11例(57.9%)。前距腓韧带腓骨起点至腓骨前部结节平均距离(AA)为17.1±3.00 mm,至腓骨隐匿结节(AO)平均距离为5.1±1.69 mm,至腓骨尖(AT)平均距离为14.1±2.86 mm,前距腓韧带距骨止点至距骨上下关节面的平均距离分别为11.4±2.25 mm及18.4±2.30 mm,至距骨前外软骨面的平均距离为4.8±1.42 mm。跟腓韧带(CFL)平均长度为31.4±3.55 mm,跟腓韧带腓骨起点至前距腓韧带腓骨起点的平均距离为6.4±2.55 mm,跟腓韧带与前距腓韧带间夹角为116.6±12.69°,跟腓韧带跟骨止点至跟骨外侧结节(CP)平均距离为15.4±2.86 mm,至跟骨后上缘(CC)平均距离为13.9±2.46 mm,至距下关节面(CS)平均距离为15.2±3.21 mm。以变异度衡量各解剖标志相对稳定性结果如下:ATFL腓骨止点AA(17.54%)<AT(20.28%)<AO(33.14%),CFL跟骨止点CC(17.70%)<CP(18.57%)<CS(21.1%)。结论:通过解剖研究发现踝关节外侧副韧带形态参数及起止点至各解剖骨性标志的距离存在一定的变异性,为临床上解剖重建踝关节外侧副韧带治疗慢性踝关节不稳定提供了解剖依据。
踝关节外侧副韧带;前距腓韧带;跟腓韧带;解剖;变异系数
踝关节扭伤占所有运动损伤的10%~15%[1,2],即使通过及时治疗,仍有近30%左右的踝关节扭伤可能发展为慢性踝关节不稳定[3]。踝关节扭伤时的主要损伤结构是踝关节外侧副韧带,包括前距腓韧带(anterior talofibular ligament,ATFL)、跟腓韧带(calcaneofibular ligament,CFL)、后距腓韧带(posterior talofibular liga⁃ment,PTFL)和外侧距跟韧带(lateral talocalcaneal liga⁃ment,LTCL)[4],其中ATFL单独损伤占80%左右,而AT⁃FL合并CFL损伤占20%左右[5]。大部分需要手术治疗的ATFL损伤可以通过改良的Broström法进行修补[6],对于修补失败、韧带残端不足、体重过大、全身韧带松弛综合征及需要尽快重返运动的患者,则需要使用自体或异体的肌腱重建踝关节外侧副韧带[7,8]。近年来,通过踝关节镜镜下重建踝关节外侧副韧带的微创手术方法在临床上也被逐渐推广[9,10],从而对于踝关节韧带形态和起止点位置的解剖定位有了更高的要求。本研究通过对人体踝关节标本外侧副韧带的精细解剖,明确踝关节外侧副韧带相关形态参数及其起止点足印区至各解剖标志的距离,为踝关节外侧副韧带重建手术提供相应依据。
1 材料与方法
本次研究选取冰冻人体下肢标本19例,其中男性10例,女性9例,年龄48~81岁(平均62.4岁)。所有标本均无手术史、骨折史或严重畸形等可能影响解剖测量的因素。
解剖开始前提前半天解冻标本,逐层切开并剥离皮肤、筋膜、肌肉,观察并切断伸肌支持带及腓骨肌腱,暴露踝关节外侧副韧带,测量并记录大体标本、前距腓韧带(ATFL)和跟腓韧带(CFL)的形态参数:(1)标本足长、内踝高、外踝高;(2)ATFL的长度(双束则分别测量)、腓骨端宽度、中部宽度、距骨端宽度、厚度、分束;(3)CFL的长度、宽度、厚度、CFL与ATFL的角度。长度测量使用精度为0.01 mm的电子游标卡尺,角度测量使用精度为1°的量角器,所有测量踝关节均处于中立位。
测量结束后分别切断ATFL和CFL,暴露其起止点足印区并标记,测量并记录ATFL和CFL各起止点足印区中心至各解剖标志的距离(图1):
(1)ATFL腓骨起点至腓骨前部结节的距离(AT⁃FL-Anterior tubercle of fibula,AA);
(2)ATFL腓骨起点至腓骨隐匿结节的距离(AT⁃FL-Obscure tubercle,AO);
(3)ATFL腓骨起点至腓骨尖的距离(ATFL-Tip of the fibula,AT);
(4)ATFL距骨止点至距骨上下关节面的距离;
(5)ATFL距骨止点至距骨前外软骨面的距离;
(6)CFL腓骨止点与ATFL腓骨止点之间的距离;
(7)CFL跟骨止点至跟骨外侧结节的距离(CFLPeroneal tubercle,CP);
(8)CFL跟骨止点至跟骨后上缘的距离(CFL-posterior superior surface of calcaneus,CC);
(9)CFL跟骨止点至距下关节面的距离(CFLSubtalar joint,CS)。
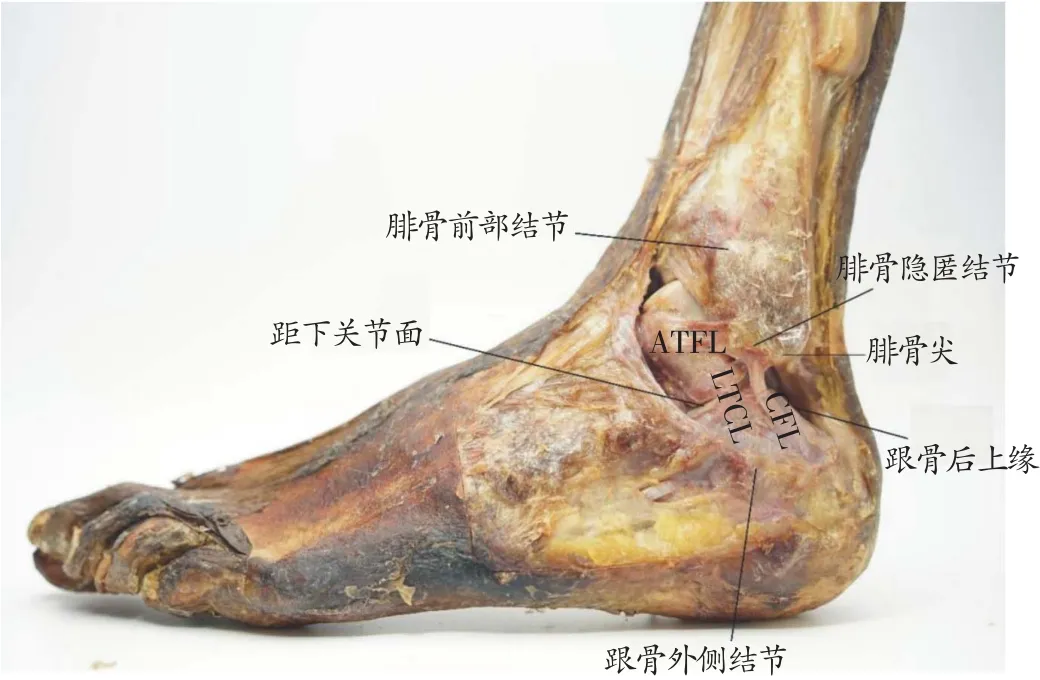
图1 ATFL:距腓前韧带;CFL:跟腓韧带;LTCL:外侧距跟韧带
图像记录使用SONYα-7II数码相机及ZEISS FE 55mm F18镜头,所有解剖由同一位操作者完成,测量分别由两位观察者独立测量,每位观察者测量3次,选择ATFL长度、ATFL与CFL之间角度及ATFL至腓骨尖距离(AT)三组数据计算观察者内及观察间相关系数并做统计检验,统计时取所有测量数据的平均值。数据统计分析使用IBM SPSS 22.0软件,计算各数值平均值、标准差,计算并比较止点至不同解剖标志距离的变异度。
2.1 可信度分析
实验开始前所有观察者经过讨论和业务学习达成解剖测量的共同操作规范,明确各解剖标志的特点,长度测量以韧带起止点中心为准。选择ATFL长度、AT⁃FL与CFL间角度和ATFL至腓骨尖距离(AT)三组数据做可信度分析。结果显示,所有观察者内(ICC1)及观察者间相关系数(ICC2)均大于0.75,说明测量方法可信度较好。见表1。
2 结果
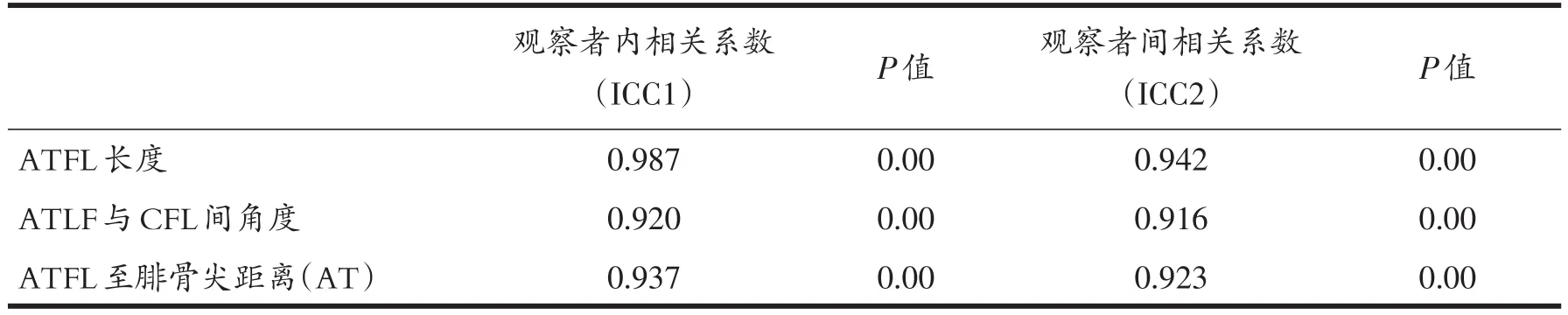
表1 数据测量的可信度分析
2.2 形态参数
本组中共19例下肢足踝标本,平均足长223.2±17.23 mm,平均内踝高80.5±5.94 mm,平均外踝高71.0±8.10 mm。
前距腓韧带呈扁平状,四方形,起自腓骨尖前上方,向前内走行,止于距骨体胫距关节面前下方。11例(57.9%)ATFL分为双束,上下两束走行基本一致,8例(42.1%)仅为单束。本组标本平均ATFL长度为23.1±2.98 mm(若双束则计算上束长度,下同),双束ATFL中下束的平均长度为17.7±2.59 mm。ATFL腓骨端宽度为7.6±1.84 mm,中部宽度为5.8±1.11 mm,距骨端宽度为8.4±1.68 mm,平均厚度为0.9±0.38 mm。跟腓韧带稍粗呈圆柱状,起自腓骨尖偏内侧,较ATFL腓骨起点更靠近腓骨尖,止于跟骨外侧面偏后方。本组标本平均CFL长度为31.4±3.55 mm,平均宽度为4.2±1.78 mm,平均厚度为1.4±0.39 mm。见表2。

表2 前距腓韧带和跟腓韧带的形态学参数(单位:mm)
2.3 起止点至解剖标志的距离
前距腓韧带腓骨起点至腓骨前部结节的平均距离(AA)为17.1±3.00 mm,至腓骨隐匿结节的平均距离(AO)为5.1± 1.69 mm,至腓骨尖的平均距离(AT)为14.1±2.86 mm。
前距腓韧带距骨止点至距骨胫距关节面的距离为11.4±2.25 mm,至距下关节面的距离为18.4±2.30 mm,至距骨前外软骨面的距离为4.8±1.42 mm。
跟腓韧带腓骨起点与前距腓韧带腓骨起点中心点之间的距离为6.4±2.55 mm,平均夹角为116.6±12.69°。跟腓韧带跟骨止点至跟骨外侧结节的平均距离(CP)为15.4±2.86 mm,至跟骨后上缘的平均距离(CC)为13.9±2.46 mm,至距下关节面的平均距离(CS)为15.2 ± 3.21 mm。
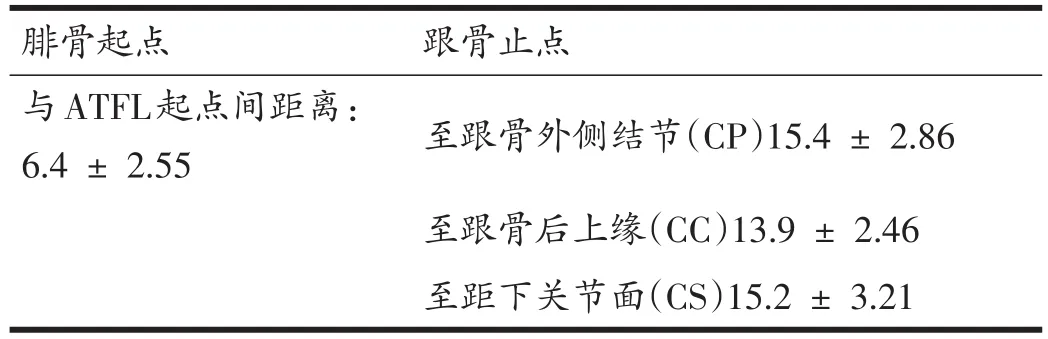
表4 跟腓韧带起止点至各解剖标志的距离(单位:mm)
以变异度衡量各解剖标志相对稳定性结果如下:ATFL腓骨起点 AA(17.54%)<AT(20.28%)<AO(33.14%),CFL跟骨止点CC(17.70%)<CP(18.57%)<CS(21.1%)。
3 讨论
踝关节外侧副韧带损伤导致的慢性踝关节不稳若保守治疗效果不佳,常需要手术治疗。无论是术前利用核磁共振或超声对韧带损伤做出诊断,还是手术中对于韧带止点的判断,以及关节镜手术入路以及重建方式的改进,都需要对踝关节外侧副韧带的解剖做更加精细的解剖及量化。本次研究对踝关节外侧副韧带的解剖测量,为相关临床诊疗的优化提供了必要的依据。
本组19例标本中,前距腓韧带呈双束的有11例(57.9%),呈单束的有8例(42.1%),单束与双束的比例与Clanton等研究结果较一致(单束50%,双束50%)[11]。Taser等研究结果显示单束为97.6%,双束仅为2.4%[12],Wenny等研究甚至表明单束比例为 100%[13],与本研究结果相差较大,可能与解剖的精细程度差异有关。本次解剖研究过程中发现部分双束ATFL在关节囊和筋膜剥离不彻底时可能与单束ATFL形态相似,若仔细清除表面筋膜后则可发现两束之间的天然间隙。Matsui等针对多篇踝关节外侧副韧带的解剖文献所做的定量综述显示[14],单束比例为61.6%,双束比例为35.7%,三束比例为2.7%,本次研究样本量较小,未发现ATFL分为三束的情况。
本组标本平均ATFL长度为23.1±2.98 mm,与Taser等研究结果[12](22.37±2.50 mm)和Burks等研究结果[15](24.8 mm)较一致,但较Milner等研究结果[16](13 mm)更长,较Testut等研究结果[17](30~40 mm)更短。已有的部分研究测量韧带长度时选取了韧带纤维最远端进行测量[14],可能导致结果较大,但起止点足印区中心点间的距离对于指导临床上解剖重建踝关节外侧副韧带更有意义。大部分研究采用直接测量起止点间的距离[11,12,15],然而本次研究中发现,前距腓韧带中立位时在距骨侧呈现“L”型转角,直接测量起止点的距离可能导致结果偏小,因此测量时采取分段测量的方式,分别测量腓骨起点和距骨止点至韧带转角的距离再行相加,因此结果较类似研究可能稍大。
研究中测量ATFL腓骨起点时选定的三个解剖标志为:腓骨前部结节、腓骨隐匿结节及腓骨尖。其中腓骨隐匿结节为腓骨尖前方数毫米一可以扪及的圆形结节,在腓骨前部结节之下,Matsui等研究显示腓骨隐匿结节可以作为ATFL和CFL在腓骨侧起点的重要参考[18]。本次研究中测得ATFL腓骨起点至各解剖标志的距离为:前距腓韧带腓骨起点至腓骨前部结节平均距离(AA)为17.1 ± 3.00 mm,至腓骨隐匿结节(AO)平均距离为5.1±1.69 mm,至腓骨尖(AT)平均距离为14.1±2.86 mm,AA的测量结果与Taser等研究结果较一致(20 ± 3.54 mm)[12],AO的测量结果与Matsui等研究结果基本一致(3.7 mm)[18],AT的测量结果与Clan⁃ton等研究较一致(双束16.3 mm,单束13.8 mm)[11]。手术中若存在韧带残端不足等情况需要重建ATFL,韧带的止点则需要通过解剖定位的数据来选择,稳定性较好的解剖标志能帮助外科医生更好地定位,由于三个测量距离的平均值差异较大,故采用变异度来衡量ATFL腓骨起点至各解剖标志距离的相对稳定性,结果如下:AA(17.54%)<AT(20.28%)<AO(33.14%)。腓骨前部结节及腓骨尖均为相对稳定的解剖标志,ATFL腓骨起点至腓骨隐匿结节的距离虽然变异度稍大,但由于平均值较小,定位误差也相对较小,且对于镜下重建有更重要的临床意义。
本次研究测得的平均CFL长度31.4±3.55 mm,与Taser等研究结果[12](31.94±3.68 mm)较一致,较Clanton等研究结果(24.7 mm)[11]稍长,可能的原因是CFL跟骨止点足印区解剖清理时远端纤维较致密且与表面筋膜较难分离,对于止点最远端位置的判断可能因不同解剖操作者的认知不同而存在一定差异。
研究中测量CFL跟骨止点时选定的三个解剖标志为跟骨外侧结节、跟骨后上缘及距下关节面。跟骨外侧结节为腓骨肌腱在CFL跟骨止点前下方走行沿线的骨性突起。本次研究中测得CFL跟骨止点至各解剖标志距离为:跟腓韧带跟骨止点至跟骨外侧结节(CP)15.4±2.86 mm,至跟骨后上缘(CC)平均距离为13.9±2.46 mm,至距下关节面(CS)平均距离为15.2±3.21 mm。CP的测量结果与Clanton等研究结果(16.3 mm)较一致[11],CC的测量结果与Taser等研究结果(12.86±2.61 mm)[12]较一致,CS的测量结果与Burks等研究结果(13 mm)[15]及Sindel等研究结果(12.8 ±1.61 mm)[19]较一致,变异度衡量结果如下CC(17.70%)<CP(18.57%)<CS(21.1%),三者相差不大。Clanton认为跟骨外侧结节是可行性最好的CFL跟骨止点定位标志[11],其在手术中较易扪及。而距下关节面相比其余二者在关节镜下更容易被观察,在镜下重建CFL时利用距下关节面对CFL跟骨止点进行定位可行性更好。
4 结论
本研究通过精细解剖发现踝关节外侧副韧带形态参数及起止点至各解剖骨性标志的距离存在一定的变异性,为临床上解剖重建踝关节外侧副韧带治疗慢性踝关节不稳定提供了解剖学依据。
[1] Lassiter TE Jr,Malone TR,Garrett WE Jr.Injury to the lateral ligaments of the ankle[J].Orthop Clin North Am,1989,20:629-640.
[2] MacAuley D.Ankle injuries:same joint,different sports[J].Med Sci Sports Exerc,1999,31:409-411.
[3] Sammarco VJ.Complications of lateral ankle ligament re⁃construction[J].Clin Orthop Relat Res,2001,391:123-132.
[4] Colville MR.Surgical treatment of the unstable ankle[J].J Am Acad Orthop Surg,1998,6(6):368-377.
[5] Kumai T,Takakura Y,Rufai A,et al.The functional anat⁃omy of the human anterior talofibular ligament in rela⁃tion to ankle sprains[J].J Anat,2002,200:457-465.
[6] Gould N,Seligson D,Gassman J.Early and late repair of lateral ligament of the ankle[J].Foot Ankle,1980,2:84-89.
[7] Krips R,van Dijk CN,Halasi T,et al.Anatomical recon⁃struction versus tenodesis for the treatment of chronic an⁃terolateral instability of the ankle joint:a 2-to 10-year follow-up,multicenter study[J].Knee Surg Sports Trauma⁃tol Arthrosc,2000,8(3):173-179.
[8] Matheny LM.Activity Level and Function after Lateral Ankle Ligament Repair Versus Reconstruction[J].Am J Sports Med,2016,44(5):1301-1308.
[9] Guillo S,Cordier G,Sonnery-Cottet B,et al.Anatomical reconstruction of the anterior talofbular and calcaneofbu⁃lar ligaments with an all-arthroscopic surgical technique[J].Orthop Traumatol Surg Res,2014,100:413-417.
[10]Lui TH.Arthroscopic-assisted lateral ligamentous recon⁃struction in combined ankle and subtalar instability[J].Arthrosc J Arthrosc Relat Surg,2007,23:554-555.
[11]Clanton TO,Campbell KJ,Wilson KJ,et al.Qualitative and quantitative anatomic investigation of the lateral an⁃kle ligaments for surgical reconstruction procedures[J].J Bone Joint Surg Am,2014,96:e98(1-8).
[12]Taser F,Shafq Q,Ebraheim NA.Anatomy of lateral an⁃kle ligaments and their relationship to bony landmarks[J].Surg Radiol Anat,2006,28:391-397.
[13]Wenny R,Duscher D,Meytap E,et al.Dimensions and at⁃tachments of the ankle ligaments:evaluation for ligament reconstruction.Anat Sci Int,2015,90:161-171.
[14]Matsui K.Anatomy of anterior talofibular ligament and calcaneofibular ligament for minimally invasive surgery:a systematic review[J].Knee Surg Sports Traumatol Ar⁃throsc DOI 10.1007/s00167-016-4194-y.published on⁃line:13 June 2016.
[15]Burks RT,Morgan J.Anatomy of the lateral ankle liga⁃ments.Am J Sports Med,1994,22:72-77.
[16]Milner CE,Soames RW.Anatomy of the collateral liga⁃ments of the human ankle joint.Foot Ankle Int,1998,19:757-760.
[17]Yildiz S,Yalcin B.The anterior talofibular and calcaneo⁃fibular ligaments:an anatomic study[J].Surg Radiol Anat,2013,35(6):511-516.
[18]Matsui K.Bony landmarks available for minimally inva⁃sive lateral ankle stabilization surgery:a cadaveric ana⁃tomical study[J].Knee Surg Sports Traumatol Arthro DOI 10.1007/s00167-016-4218-7.published online:28 June 2016.
[19]Sindel M.Anatomy of the lateral ankle ligaments[J].Turk JMed Sci,1998,28:53-56
Anatom ical Landmarks for Lateral Ankle LigamentReconstruction—a Cadaveric Study
Ma Kui,Hua Yinghui,LiHongyun,Zhang Jian,Chen Shiyi
DepartmentofSportsMedicine,Huashan Hospital,Fudan University,Shanghai200040,China
Hua Yinghui,Email:hua023@hotmail.com
Purpose To clarify the morphological parameter and describe the distance from the inser⁃tion of the lateral ankle ligaments to the adjacent bony landmarks through precisely anatomical explore of human cadaveric ankles,so as to provide anatomical evidences for the reconstruction of lateral ankle ligaments.Methods Nineteen ankle specimens were dissected to isolate the lateral ankle ligaments and measure the morphological parameters such as length,width,thickness and the distance from the inser⁃tion of the lateral ankle ligaments to the adjacent bony landmarks.Results The average length of ante⁃rior talofibular ligaments(ATFL)was 23.1 ± 2.98 mm,among which 8 were single-banded(42.1%)and 11 were double-banded(57.9%).The average distance from the fibular origination of ATFL to the ante⁃rior tubercle of fibula(AA)was 17.1 ± 3.00 mm,to the fibular obscure tubercle(AO)was 5.1 ± 1.69 mm,to the tip of the fibula(AT)was 14.1 ± 2.86 mm.The distances from the talus insertion of ATFL to the superior and inferior talus articular surface were 11.4±2.25 mm and 18.4±2.30 mm respec⁃tively,to the anterior lateral talus chondral surface was 4.8 ± 1.42 mm.The average length of calcaneo⁃fibular ligament(CFL)was 31.4 ± 3.55 mm.The average distance of the fibular origination from ATFL to CFL was 6.4 ± 2.55 mm.The average angle between ATFL and CFL was 116.6 ± 12.69°.The dis⁃tance from the calcaneus insertion of CFL to the peroneal tubercle(CP)was 15.4 ± 2.86 mm,to the pos⁃terior superior border of calcaneus(CC)was 13.9 ± 2.46 mm,to the subtalar joint surface was 15.2 ±3.21 mm.The coefficient variation assessing the anatomical reliability of different bony landmarks were as follows:ATFL fibular origination AA(17.54%)<AT(20.28%)< AO(33.14%),CFL calcaneus inser⁃tion CC(17.70%)<CP(18.57%)<CS(21.1%).Conclusion Certain variations exist in the morphological parameters and the distances from the insertion of the lateral ankle ligaments to the adjacent bony landmarks.It provides anatomical evidence for lateral ankle ligament reconstruction in treating chronic ankle instability.
lateral ankle ligament,anterior talofibular ligaments(ATFL),calcaneofibular ligament(CFL),dissection,coefficient variation(CV)
2017.02.28
国家自然科学基金面上项目(8157090042)
第1作者:马魁,Email:makui6210@163.com;
华英汇,Email:hua023@hotmail.com



