何国彬 吴巧杏 吴起



【摘要】 目的:探讨桡骨近端骨折的损伤机制与骨折类型和合并伤的关系。方法:回顾性分析2014年1月-2018年12月本院就诊的50例桡骨近端骨折患者的临床资料。采用Mason分型对骨折类型进行区分,探讨桡骨近端骨折的损伤机制与骨折类型和合并伤的关系。结果:不同骨折类型的手部着地,外翻位摔倒情况比较,差异有统计学意义(P<0.05),且此损伤机制下以Ⅱ型骨折为主。不同骨折类型的肘部直接着地、跌落前受到强力牵拉以及硬物撞击情况比较,差异均无统计学意义(P>0.05)。不同损伤机制对是否伴有合并伤比较,差异有统计学意义(P<0.05)。结论:手部着地、外翻位摔倒是桡骨近端骨折的主要损伤机制,且损伤机制与伴有合并伤有关。
【关键词】 桡骨小头 桡骨颈 桡骨近端骨折 损伤机制
Relationship between Injury Mechanism of Proximal Radius Fracture and the Fracture Types and Complicated Injuries/HE Guobin, WU Qiaoxing, WU Qi. //Medical Innovation of China, 2021, 18(23): -170
[Abstract] Objective: To explore the relationship between the injury mechanism of the proximal radius fracture and the fracture types and complicated injuries. Method: The clinical data of 50 patients with proximal radius fracture treated in our hospital from January 2014 to December 2018 were retrospectively analyzed. The Mason classification was used to distinguish the fracture types and to explore the relationship between the injury mechanism of the proximal radius fracture and the fracture types and complicated injuries. Result: There was significant difference in valgus fall among different fracture types (P<0.05), and type Ⅱ fracture was the main injury mechanism. There were no significant differences in the direct landing, the strong pulling before falling and the impact of hard objects on the elbow of different fracture types (P>0.05). There was significant difference among different injury mechanisms in the combination of injuries (P<0.05). Conclusion: Hand landing and valgus fall are the main injury mechanism of the proximal radius fracture, and the injury mechanism is related to the complicated injuries.
[Key words] Radial capitulum Radial neck Proximal radius fracture Injury mechanism
First-author’s address: Leliu Hospital Affiliated to Shunde Hospital of Guangzhou University of Traditional Chinese Medicine, Foshan 528322, China
doi:10.3969/j.issn.1674-4985.2021.23.041
桡骨近端骨折是较为常见的肘关节损伤,并常伴有不同程度的软组织损伤[1-3]。近端桡骨包括盘状的桡骨小头和桡骨颈。桡骨小头上面为凹面,其直径略大于肱骨小头的直径,与肱骨小头形成肱桡关节,使得肱尺关节能自由活动。环绕在桡骨小头环状关节面的为环状韧带,其附着于尺骨并与桡尺骨紧密连接在一起,功能为使桡骨小头在其内部旋转,且在肘关节屈曲时避免桡骨小头脱位[4-9]。肘关节内侧副韧带(MCL)的前侧束是维持肘关节外翻稳定性的主要结构,桡骨近端骨折易造成MCL损伤,从而严重影响肘关节的稳定性[10-13]。桡骨近端骨折主要是摔倒后患者手掌撑地,此时前臂旋前且肘关节伸直,外翻力量轴向传递至肘关节,使桡骨小头与肱骨头发生撞击,从而造成桡骨小头或桡骨颈发生骨折,严重者还伴有MCL撕裂及肘关节脱位。桡骨近端骨折主要以桡骨小头骨折最为常见,而桡骨小头骨折约有10%伴有肘关节的脱位,以及侧韧带损伤[14-15]。对于桡骨近端骨折处理方法较多,临床关于其治疗方法的选择存在较大争议,但其骨折形态的确认是恰当选择处理方法的前提条件。目前临床主要借助于X射线、CT以及核磁手段对骨折类型进行诊断,而由于不同的检查手段侧重点不同,且存在漏诊及误诊等情况,临床较为复杂的情况需结合不同的手段综合判断,从而造成患者等待时间较长。本文拟通过对桡骨近端骨折的损伤机制与骨折类型和合并伤的关系进行分析,以期为临床判断骨折类型、迅速做出治疗方案、提高判断疾病预后等提供参考依据。
1 资料与方法
1.1 一般资料 回顾性分析2014年1月-2018年12月本院就诊的50例桡骨近端骨折患者的临床资料。(1)诊断标准:①典型症状为肘部后外侧呈红肿,且有疼痛感,肘关节行旋转、屈伸等活动时疼痛加剧;②以肘关节正侧位进行X射线等常规检查为主,必要时进行CT检查,并结合MRI对是否发生MCL或环状韧带等软组织损伤进行辅助诊断。(2)骨折分类:骨折分类以Mason分型,Ⅰ型为骨折无移位;Ⅱ型为骨折有分离移位,骨折块有大小,有时小骨折块嵌如关节间隙或游离于肱桡关节外侧缘;Ⅲ型为桡骨头粉碎性骨折,桡骨头呈粉碎状,移位或无移位;Ⅳ型为桡骨小头骨折并肘关节脱位。(3)纳入标准:①年龄7~58岁;②经医师诊断为桡骨近端骨折。(4)排除标准:①合并心、肺、胃肠功能疾病;②合并高血糖、高血压;③入组前6个月内接受过腹部相关手术。本研究已经获得医院医学伦理委员会批准,且受试者均已签署书面知情同意书。
1.2 方法 对开放性损伤进行清创。根据骨折类型、骨折移位大小、骨折片段数及大小、粉碎程度、关节稳定性、前臂内旋及外旋程度等,进行切开复位内固定治疗、桡骨头切除术或进行桡骨头置换。对合并肘关节脱位者行手法复位。
1.3 观察指标 (1)观察不同骨折部位患者的一般资料。(2)比较不同骨折类型的损伤机制。(3)分析损伤机制与合并伤的关系。
1.4 统计学处理 采用SPSS 20.0软件对所得数据进行统计分析,计数资料以率(%)表示,比较采用χ检验;计量资量用(x±s)表示。以P<0.05为差异有统计学意义。
2 结果
2.1 不同骨折部位患者的一般资料 桡骨头骨折患者年龄19~58岁,平均(30.27±1.81)岁;桡骨颈骨折患者年龄7~42岁,平均(22.13±3.82)岁。纳入患者一般资料情况见表1。有2例患者为肘关节骨折恐怖三联征,其影像检测结果见图1。
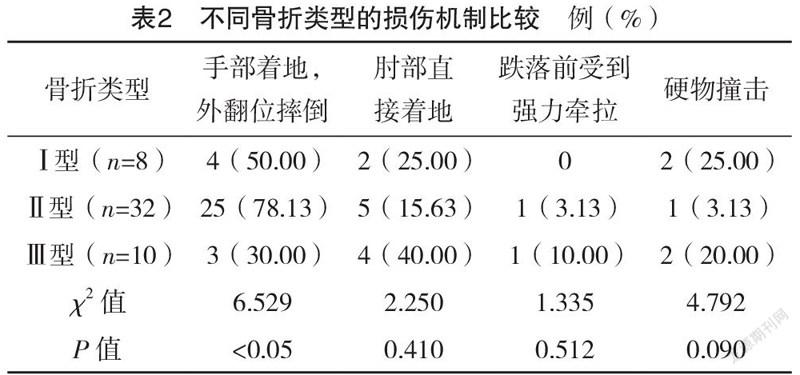
2.2 不同骨折类型的损伤机制比较 不同骨折类型的手部着地,外翻位摔倒情况比较,差异有统计学意义(P<0.05),且此损伤机制下以Ⅱ型骨折为主。不同骨折类型的肘部直接着地、跌落前受到强力牵拉以及硬物撞击情况比较,差异均无统计学意义(P>0.05)。见表2。
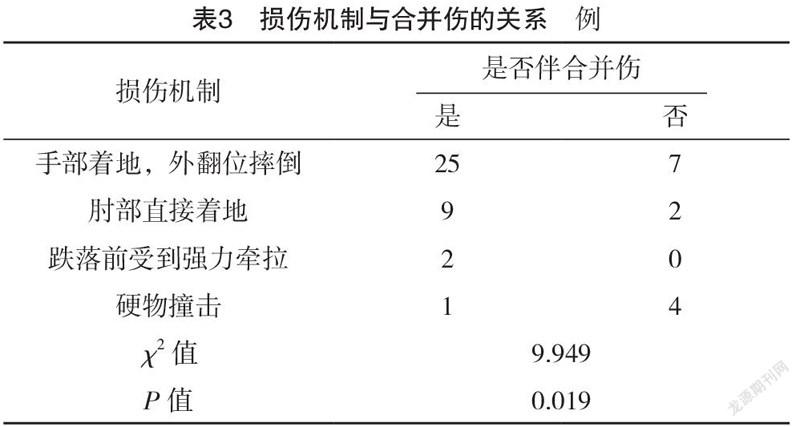
2.3 损伤机制与合并伤的关系 不同损伤机制的是否伴有合并伤比较,差异有统计学意义(P<0.05),见表3。
3 讨论
桡骨近端与桡骨干形成一定的角度,约为15°,近端组成包括桡骨小头及桡骨颈。桡骨近端骨折包括桡骨颈骨折及桡骨小头骨折,由于儿童桡骨小骨仍为软骨,桡骨颈骨折更多见于儿童,但桡骨小头骨折在成人中更常见,约有20%的肘关节骨折为桡骨小头骨折。本文中纳入的50例患者,40例患者为桡骨小头骨折,10例患者为桡骨颈骨折,其中13例患者位有脱位。损伤原因以前臂旋前伸展位摔伤为主,这与文献[16-17]报道的桡骨近端骨折及脱位的主要致伤原因一致。当摔倒时,多数人出于保护意识会采用手掌撑地的方式以避免、减少对身体其他部位的损伤,此时肘关节提携角则可导致较大的外翻应力的轴向传导,这时肱骨小头则对桡骨小头产生撞击力,最终使桡骨小头发生骨折。因而损伤机制中以手部着地、外翻位摔倒最为常见,且通过本文的研究显示,不同骨折类型的手部着地,外翻位摔倒情况比较,差异有统计学意义(P<0.05),且此损伤机制下以Ⅱ型骨折为主。不同骨折类型的肘部直接着地、跌落前受到强力牵拉以及硬物撞击情况比较,差异均无统计学意义(P>0.05)。不同损伤机制的是否伴有合并伤比较,差异有统计学意义(P<0.05)。易造成Ⅱ型骨折以及韧带损伤、肘关节脱位等合并伤。提示在临床工作中患者如以前臂旋前伸展位摔伤,而且损伤机制为手部着地、外翻位摔倒的情况,则应及时进行CT、MRI等检查,对骨折形态、合并伤情况及时了解,以便制定出恰当的处置方法,最大程度缓解患者痛苦,降低损伤对患者生活能力及生活质量的不良影响[18-19]。
恐怖三联征是指桡骨小头骨折,而同时尺骨冠状骨折,并伴有肘关节向后脱位,一般情况还可能合并肘关节外侧或者内侧副韧带损伤,是最严重的肘关节损伤类型[20-21]。当前臂处于旋后状态时,轴向力作用于前臂,肘关节处于外展位从而产生压缩剪切力。临床中恐怖三联征愈合效果较差,且易产生创伤性关节炎等并发症,从而影响预后[22]。本研究中有2例患者为恐怖三联征患者,一例为58岁女性,一例为27岁男性,均为跌落伤,着地时为手部撑地、外翻位倒地。本研究中对于上述两位均以内固定术处置,以避免桡骨头切除术等引起的并发症,术后至出院前患者恢复情况较好,还需进一步跟踪恢复情况。此外,笔者在临床中治疗桡骨近端骨折时以恢复解剖学结构、实现肘关节进行无痛且稳定的运动、避免关节创伤导致的退行性改变及其他并发症。综合骨折类型、关节损伤情况及合并损伤情况,选择治疗手段。对于临床肘关节骨折伴脱位时,建议修复或重建桡骨近侧,以保持肘关节内翻、外翻稳定性,减少尺侧副韧带的应力,从而可有效防止近端桡骨移位。本研究虽对桡骨近端骨折损伤机制与骨折类型及合并伤的相关性进行了分析,但纳入病例数较少,且不能实际掌握患者实际损伤的真实情况,因此尚难以实现根据损伤机制对骨折形态进行一定程度的预判。后期研究中将对病例数进行扩大,同时根据实际损伤事件、结合生物力学原理,对损伤机制进行深入探讨,以期为骨折类型的预判以及如何在应急事件中最大限度地避免非必要骨折损伤提供参考。
综上所述,手部着地、外翻位摔倒是桡骨近端骨折的主要损伤机制,且损伤机制与伴有合并伤有关。
参考文献
[1] Griffin M,Roushdi I,Osagie L,et al.Patient-Reported Outcomes Following Surgically Managed Perilunate Dislocation:Outcomes After Perilunate Dislocation[J].Hand,2016,11(1):22-28.
[2] Capo J T,Shamian B,Francisco R,et al.Fracture pattern characteristics and associated injuries of high-energy,large fragment,partial articular radial head fractures:a preliminary imaging analysis[J].Journal Orthop Traumatol,2015,16(2):125-131.
[3] Lacheta L,Siebenlist S,Lauber M,et al.Proximal radius fracture morphology following axial force impact:a biomechanical evaluation of fracture patterns[J].BMC Musculoskelet Disord,2019,20(1):147.
[4] Leschinger T,Muller L P,Hackl M,et al.The cortical irregularity in the transition zone of the radial head and neck:a reliable radiographic sign of an occult radial head fracture[J].Archives of Orthopaedic & Trauma Surgery,2016,136(8):1115-1120.
[5] Malone P S C,Shaw O G,Lees V C.Anatomic Relationships of the Distal and Proximal Radioulnar Joints Articulating Surface Areas and of the Radius and Ulna Bone Volumes-Implications for Biomechanical Studies of the Distal and Proximal Radioulnar Joints and Forearm Bones[J].Frontiers in Bioengineering and Biotechnology,2016,4(S1):61.
[6] Chytas I D,Antonopoulos C,Cheva A,et al.Capitellar Erosion after Radial Head Arthroplasty:A Comparative Biomechanical Study of Operated Radial Head Fractures on Cadaveric Specimens[J].Orthopaedics & Traumatology Surgery & Research,2018,104(6):853-837.
[7] Rausch V,Wegmann S,Hackl M,et al.The radial head size in relation to osseous landmarks of the forearm[J].Surgical Radiologic Anatomy,2019,41(4):415-421.
[8] Walid O,Meriem B,Zeineb A,et al.An Uncommon Combination of Fractures around the Elbow:Capitellum Fracture Associated with Radial Head Fracture[J].Journal of Orthopaedic Case Reports,2016,6(4):108-110.
[9] Schamall M,Pietschmann U,Moser A,et al.Diagnosis of contact injuries in a mediaeval skeleton analysed by µCT and histology[J].Wiener Medizinische Wochenschrift,2012,162(17-18):386-393.
[10] Are A,Tornatore I,Theodorakis E.Operative management of a shear fracture of the bilateral capitellum:A case report and review of the literature[J].Chinese Journal Traumatology,2016,19(4):231-234.
[11] Rausch V,Konigshausen M,Schildhauer T A,et al.Fractures of the capitellum humeri and their associated injuries[J].Obere Extrem,2018,13(1):33-37.
[12] Hackl M,Burkhart K J,Wegmann K,et al.From radial head to radiocapitellar to total elbow replacement:A case report[J].International Journal Surgery Case Reports,2015,15(1):35-38.
[13] Zhang F Y,Wang X D,Zhen Y F,et al.Treatment of Severely Displaced Radial Neck Fractures in Children with Percutaneous K-wire Leverage and Closed Intramedullary Pinning[J/OL].Medicine (Baltimore),2016,95(1):e2346.
[14] Wang J,Qi W,Shen X,et al.Results of arthroscopic fixation of Mason type Ⅱ radial head fractures using Kirschner wires[J/OL].Medicine (Baltimore),2018,97(12):e0201.
[15] Kaiser M,Eberl R,Castellani C,et al.Judet type-Ⅳ radial neck fractures in children:Comparison of the outcome of fractures with and without bony contact[J].Acta Orthopaedica,2016,87(5):529-532.
[16] Dei Giudici L,Faini A,Garro L,et al.Arthroscopic management of articular and peri-articular fractures of the upper limb[J].Efort Open Reviews,2017,1(9):325-331.
[17] Strafun S,Levadnyi I,Makarov V,et al.Comparative Biomechanical Analysis of Stress-Strain State of the Elbow Joint After Displaced Radial Head Fractures[J].Journal of Medical and Biological Engineering,2018,38(4):618-624.
[18] Lanting B A,Ferreira L M,Johnson J A,et al.The effect of excision of the radial head and metallic radial head replacement on the tension in the interosseous membrane[J].Bone Joint Journal,2013,95(10):1383-1387.
[19] Zhang C,Zhong B,Luo C F.Treatment strategy of terrible triad of the elbow:Experience in Shanghai 6th People’s Hospital[J].Injury,2014,45(6):942-948.
[20] Kovacevic D,Vogel L A,Levine W N.Complex elbow instability:radial head and coronoid[J].Hand Clinics,2015,31(4):547-556.
[21]蒋协远,查晔军,公茂琪,等.肘关节内翻一后内侧旋转不稳定的诊断与治疗[J].中华创伤骨科杂志,2012,4(1):3-7.
[22] Bonneville N.Radial head replacement in adults with recent fractures[J].Orthopaedics & Traumatology:Surgery & Research,2016,102(1):69-79.
(收稿日期:2020-09-21) (本文编辑:张明澜)



