郭洪亮韩亚军伊力哈木·托合提
Lisfranc损伤术后创伤性关节炎的临床研究*
郭洪亮①韩亚军①伊力哈木·托合提①
目的:评估Lisfranc损伤术后创伤性关节炎的临床研究。方法:选取本院19例伴有Lisfranc损伤的患者,其中男15例,女4例,年龄21~58岁,平均41岁。患者损伤后进行了切开复位内固定和闭合复位内固定术(采用空心螺钉和克氏针)。骨折情况:同侧7例,单独型7例,分离型5例。其中6例为开放性骨折,8例损害5个跖跗关节,6例仅有韧带损伤。采用MFS和AOFAS评分系统对结果进行评估,负重位X线片评估完全复位、半脱位、排列错乱和术后创伤性关节炎。结果:随访24~40个月,平均30个月。解剖复位组的AOFAS评分为(79.3±4.85)分,MFS评分为(80.4±4.11)分,均高于非解剖复位组的(67.5±5.13)分、(69.4±6.07)分,差异均有统计学意义(P=0.0007、P=0.0009);非解剖组的术后创伤性关节炎发生率较解剖组更易发生(P=0.037)。4例患者发展成术后创伤性关节炎,其中1例在内固定取出后发展成横向半脱位,2例患者发展成平足。2例患者有严重的功能受限,其中1例患者进行了关节融合。复合骨折的2例患者出现伤口的表面感染。3例患者出现空心钉的断裂。结论:采用解剖复位治疗Lisfranc损伤的患者,疗效较好,很少发展成关节炎。
创伤性关节炎; Lisfranc损伤; 内固定术
Lisfranc损伤比较罕见,发生率占全部骨折的0.2%,这个数字可能被低估,因为Lisfranc损伤中20%~40%被忽略或被误诊成足扭伤或单纯跖跗骨骨折[1-3]。如果不合理的治疗,严重的骨不连或者功能损害可能出现[4]。闭合复位和石膏固定可能导致差的治疗结果和重新出现移位[5-6]。解剖复位和内固定目前被公众认可,但切开复位内固定中不伴有骨折的韧带损伤也会与差的术后恢复结果联系在一起[7-10]。笔者评估空心螺钉与克氏针治疗Lisfranc损伤术后创伤性关节炎的决定危险因素。
1 资料与方法
1.1 一般资料 选取2009年11月-2012年4月本院19例伴有Lisfranc损伤的患者,其中男15例,女4例;年龄21~58岁,平均41岁;患者经历了开放/闭合复位和内固定(采用空心螺钉和克氏针),伴有Lisfranc损伤(图1)。排除瘦弱、先天性畸形、先天性神经系统疾病、挤压伤的患者。Lisfranc骨折分型:同侧(I型)7例,单独型(II型)7例,分离型(III型)5例。患者中右足损伤10例,开放性骨折6例,多重创伤3例;3例有身体同侧的下肢骨折,8例损伤5个跖跗关节,4例仅损伤了内侧柱,3例仅损伤后柱,6例单纯韧带损伤,13例骨折脱位。对于上述lisfranc损伤骨折情况不稳定的患者笔者采用切开复位内固定术(用螺钉和克氏针),这些患者被定义为在负重位X线上内侧柱排列紊乱移位>1 mm,或者骰骨和第四跖骨在斜位片上排列紊乱,或者第二跖骨和中间楔骨在正侧位X线片上丢失正常的队列[11]。

图1 Lisfranc损伤及术后复查
1.2 手术方法 肿胀消退后,患者接受治疗,所有患者先进行闭合复位,闭合复位失败后采用切开复位内固定术。在第一和第二跖骨基底之间背侧踇长伸肌腱旁侧做一个长切口,背内侧皮神经的内侧分支注意保护。如果视野紧张,切口可以延长到末端伸肌支持带[3,12]。足背动脉和腓深神经通过可伸缩性线圈游离。复位从第二跖骨楔骨关节开始[13]。然后复位跖骨基底骨折,小的不可复位的碎片被移除。开放性骨折要反复大量的冲洗。空心螺钉从内侧楔骨横向方向钉入,用克氏针和巾钳临时固定,经皮导针沿着远端到近端方向钉入,影像学控制下观察复位情况,术中直径4 mm空心螺钉被使用,术中要注意螺钉头的埋入情况,避免刺激伸肌腱。随后第一和第三跖骨楔骨关节复位用同样的方式固定,第四和第五跖跗关节的稳定性自然恢复。如果仍然不稳定,可在与第一切口平行的基础上做第二切口,用克氏针固定。在关闭伤口的过程中避免缝合线过紧。其中5例采用空心螺钉固定,4例采用克氏针固定,10例同时采用空心螺钉和克氏针固定。
术后,患者在膝关节下方打踝关节中立位石膏2周。4周内患者禁止负重。6周后克氏针取出,开始逐渐负重(图2)。空心螺钉在4个月后取出。
1.3 评价标准 疼痛、功能和外观通过MFS评分系统和AOFAS评分系统评估[12-15]。以负重位X线片评估骨不连、半脱位、排列紊乱和术后创伤关节炎。解剖对齐:在正侧位X线片跖骨的内侧缘与中间楔骨一致,在斜位片上第4跖骨的内侧缘与骰骨相一致,在斜位片上第三跖骨的外侧缘与外侧楔骨相一致,平足测量根据骰骨的跖侧缘和第四跖骨的基底部的距离。

图2 拔出克氏针后X线
1.4 统计学处理 采用SPSS 19.0统计学软件对数据进行处理,计量资料采用(±s)表示,比较采用t检验,计数资料比较采用 χ2检验,以P<0.05为差异有统计学意义。
2 结果
所有患者随访24~40个月,平均30个月。闭合复位5例患者,患者主要是仅仅损伤1个跖跗关节的患者,但闭合复位的患者均未达到解剖复位。其余14例患者均为切开复位内固定,基本达到解剖复位。所有患者MFS评分为(76.2±7.08)分,AOFAS评分为(77.5±6.73)分。解剖复位组的AOFAS评分为(79.3±4.85)分,MFS评分为(80.4±4.11)分,高于非解剖复位组的(67.5±5.13)分、(69.4±6.07)分,差异均有统计学意义(P=0.0007、P=0.0009)。骨折脱位的患者与韧带损伤的患者在MFS与AOFAS评分上比较差异无统计学意义(P>0.05)。与解剖复位组相比,非解剖复位组更容易发生后创伤性关节炎(3/5VS1/14,P=0.037),见表1。多重骨折的2例患者发展成表面感染,其中1例患者通过静脉注入抗生素行清创术。19例患者中1例患者经历了植皮手术。3例患者空心钉折断。患者均未出现深静脉血栓、疼痛性神经瘤、反射交感神经萎缩。4例患者发展成术后创伤性关节炎,其中1例在内固定物移除后发展成横向半脱位,2例患者发展成平足。2例患者有严重功能受限并发症,给予其中1例患者行关节融合。
表1 不同复位和骨折类型患者的MFS、AOFAS评分的比较(±s) 分
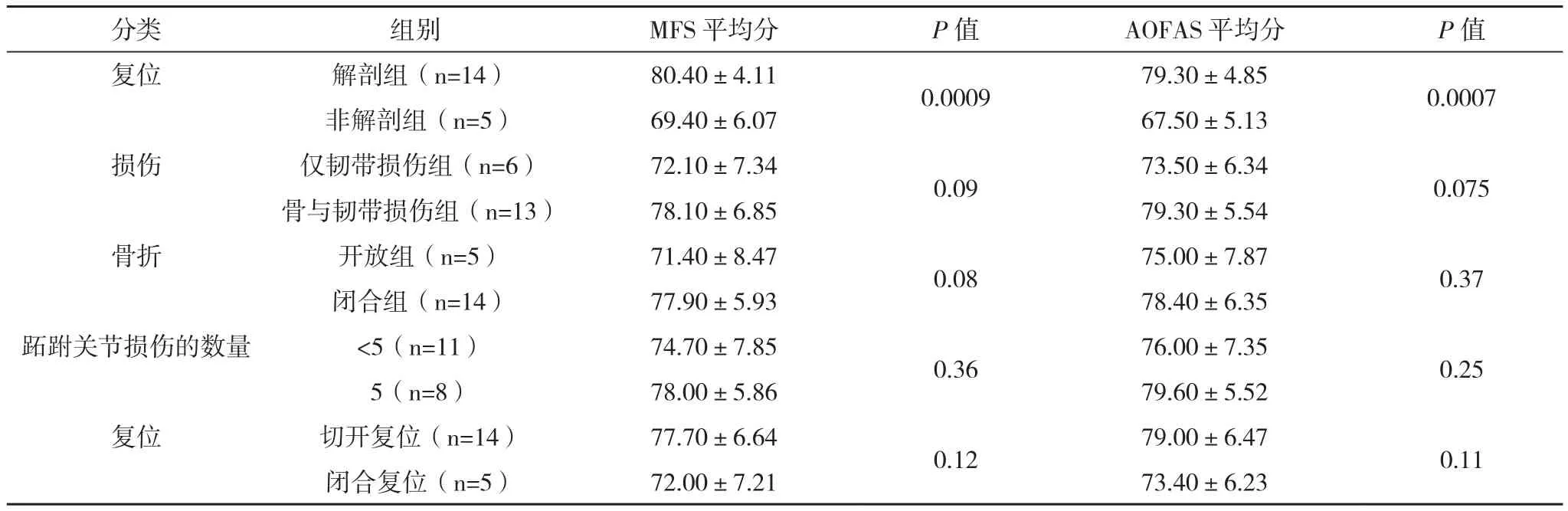
表1 不同复位和骨折类型患者的MFS、AOFAS评分的比较(±s) 分
分类 组别 MFS平均分 P值 AOFAS平均分 P值复位 解剖组(n=14) 80.40±4.11 0.0009 79.30±4.85 0.0007非解剖组(n=5) 69.40±6.07 67.50±5.13损伤 仅韧带损伤组(n=6) 72.10±7.34 0.09 73.50±6.34 0.075骨与韧带损伤组(n=13) 78.10±6.85 79.30±5.54骨折 开放组(n=5) 71.40±8.47 0.08 75.00±7.87 0.37闭合组(n=14) 77.90±5.93 78.40±6.35跖跗关节损伤的数量 <5(n=11) 74.70±7.85 0.36 76.00±7.35 0.25 5(n=8) 78.00±5.86 79.60±5.52复位 切开复位(n=14) 77.70±6.64 0.12 79.00±6.47 0.11闭合复位(n=5) 72.00±7.21 73.40±6.23
3 讨论
Lisfranc关节通过跗骨末端和跖骨及其间的韧带支撑结构共同构成复杂的骨间关系来维持中足、前足的稳定[16]。内侧楔骨和第二跖骨之间的骨间韧带众所周知被称为Lisfranc韧带,第一跖跗骨关节囊通过跖侧和背侧韧带增强,第二跖骨通过所有楔骨锁在了中间楔骨邻近的凹槽榫眼中[17]。由于趾伸肌和背侧韧带支撑力量薄弱,大多数脱位朝向背侧并且发生二次跖屈损伤[17]。当脱位发生时,跖跗关节的形状和位置倾向于足的纵向轴线压缩,跖跗关节损伤从扭伤、微妙的半脱位到全部的位移[18]。Lisfranc关节损伤后也可引起严重的跖跗关节排列紊乱[18-19]。治疗从闭合复位用或者不使用克氏针到解剖复位和使用克氏针或者空心螺钉[20-24]。由于第一、二跖骨基底跖侧斑点标记不能被广泛认知,Lisfranc损伤被频繁的忽视或者误诊[25-26]。公路交通事故普遍引起骨折损伤,然而通常引起没有骨折的脱位,损伤机制可能是直接也可能是间接的[17]。直接暴力从脚底撞击跖骨,一起横向移位。间接暴力下前足在跖侧容易改变形态出现二次骨折,足的背侧韧带的力量比跖侧韧带的力量弱,因此抵抗更少的暴力。Lisfranc损伤被分为同侧型、单独型、分离型。如果骨折不能合理的被治疗,骨不连容易发生,穿鞋也很困难。疼痛畸形可能发生[4]。稳定的解剖复位术后可以产生更好的功能结构[7-9]。内固定物选择克氏针和空心螺钉,即使在克氏针轻微较高的失败率研究中,内侧柱被空心螺钉固定,也可提供更强的更稳定的结构。然而外侧柱用克氏针固定可以保护正常的移动性,用空心螺钉严格的固定会改变正常足动力学[27-33]。
切开复位和闭合复位已经有报道[29-31]。由于全部的力量由关节软骨承担,纯粹的没有骨折的韧带损伤往往与差的术后结构相关联的,尽管切开复位和内固定的应用。在笔者的研究中,对于Lisfranc损伤的患者当中,解剖复位是对于预测患者术后的疗效的最重要的指标。解剖复位的患者很少发展成关节炎(P=0.037)并且获得更好的MAF得分和AOFAS得分(P<0.05),关节软骨的损伤,非解剖复位和不稳定的内固定可能导致术后创伤性关节炎。Lisfranc损伤内固定术后,对于取出的内固定后没有确切的时间,克氏针通常8周移除,然而空心螺钉被移除在12周~3年,或者有症状的患者[33-34]。对于连接不全性骨折,解剖复位切开复位内固定比关节融合更加具有优越性。
笔者的研究中样本小,具有限制性,对于进行大样本的进一步的学习和长时间的随访是必要的。
[1] Panchbhavi V K,Vallurupalli S,Yang J,et al.Screw fixation compared with suture-button fixation of isolated Lisfranc igament injuries[J].J Bone Joint Surg Am,2009,91(14):1143-1148.
[2] Vuori J P,Aro H T.Lisfranc joint injuries: trauma mechanisms and associated injuries[J].J Trauma,1993,35(10):40-45.
[3] Rammelt S,Schneiders W,Schikore H,et al.Primary open reduction and fixation compared with delayed corrective arthrodesis in the treatment of tarsometatarsal (Lisfranc) fracture dislocation[J].J Bone Joint Surg Br,2008,90(4):1499-1506.
[4] Mann R A,Prieskorn D,Sobel M.Mid-tarsal and tarsometatarsalarthrodesis for primary degenerative osteoarthrosis or osteoarthrosis after trauma[J].J Bone Joint Surg Am,1996,78(9):1376-1385.
[5] Curtis M J,Myerson M,Szura B.Tarsometatarsal joint injuries in the athlete[J].Am J Sports Med,1993,21(1):497-502.
[6] Komenda G A,Myerson M S,Biddinger K R.Results of arthrodesis of the tarsometatarsal joints after traumatic injury[J].J Bone Joint Surg Am,1996,78(11):1665-1676.
[7] Blanco R P,Merchan C R,Sevillano R C,et al[J].Tarsometatarsal fractures and dislocations[J].J Orthop Trauma,1998,2(3):188-194.
[8] Martin D P,Engelberg R,Agel J,et al.Development of a musculoskeletal extremity health status instrument: the musculoskeletal function assessment instrument[J].J Orthop Res,1996,14(2):173-181.
[9] Martin D P,Engelberg R,Agel J,et al.Comparison of the musculoskeletal function assessment questionnaire with the short Form-36, the western ontario and Mc Master universities osteoarthritis index, and the sickness impact profile health-status measures[J].J Bone Joint Surg Am,1997,79(9):1323-1335.
[10] Myerson M S,Fisher T,Burgess A R,et al.Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment[J].Foot Ankle,1986,6(5):225-242.
[11] Coss H S,Manos R E,Buoncristiani A,et al.Abduction stress and AP weight bearing radiography of purely ligamentous injury in the tarsometatarsal joint[J].Foot Ankle Int,1998,19(8):537-541.
[12] Canale S T,Beaty J H.Fractures and dislocations of foot[M].11th ed.In: Campbell’s Operative Orthopaedics. Philadelphia: Mosby Elsevier,2008:4876.
[13] English T A.Dislocations of the metatarsal bone and adjacent toe[J].J Bone Joint Surg Br,1964,46(1):700-704.
[14] Sanders R,Fortin P,Di Pasquale T,et al.Operative treatment in 120 displaced in traarticular calcaneal fractures. Results using a prognostic computed tomographyscan classification[J].Clin Orthop Relat Res,1993,290(1):87-95.
[15] Kitaoka H B,Alexander I J,Adelaar R S,et al.Clinical rating systems for the ankle, hindfoot, midfoot, hallux, and lesser toes[J]. Foot Ankle Int,1994,15(7):349-353.
[16] Siddiqui N A,Galizia M S,Almusa E,et al.Evaluation of the tarsometatarsal joint using conventional radiography, CT, and MR imaging[J].Radiographics,2014,34(2):514-531.
[17] Wiley J J.The mechanism of tarso-metatarsal joint injuries[J].J Bone Joint Surg Br,1971,53(3):474-482.
[18] Ismail Demirkale M D,Osman Tecimel M D,Ismail Celik M D,et al.The effect of the Tscherne injury pattern on the outcome of operatively treated Lisfranc fracture dislocations[J].Foot and Ankle Surgery,2013,19(3):188-193.
[19] Resch S,Stenstrom A.The treatment of tarsometatarsal injuries[J]. Foot Ankle,1990,11(3):117-120.
[20] Randt T,Dahlen C,Schikore H,et al.Dislocation fractures in the area of the middle foot: injuries of the Chopart and Lisfranc joint in German[J].Zentralbl Chir,1998,123(4):1257-1266.
[21] Arntz C T,Veith R G,Hansen S T.Fractures and fracturedislocations of the tarsometatarsal joint[J].J Bone Joint Surg Am,1988,70(2):173-181.
[22] Kuo R S,Tejwani N C,Digiovanni C W,et al.Outcome after open reduction and internal fixation of Lisfranc joint in juries[J].J Bone Joint Surg Am,2000,82(5):1609-1618.
[23] Richter M,Thermann H,Hufner T,et al.Aetiology, treatment and outcome in Lisfranc joint dislocations and fractured islocations[J].Foot Ankle Surg,2002,8(4):21-32.
[24] Calder J D,Whitehouse S L,Saxby T S.Results of isolated Lisfranc injuries and the effect of compensation claims[J].J Bone joint Surg Br,2004,86(4):527-530.
[25] Vivek K E,Fishman J A,Carrino L M.Epidemiology, imaging and treatment of Lisfranc fracture-dislocations revisited[J].Skeletal Radiol,2012,41(2):129-136.
[26] Rammelt S,Schneiders W,Zwipp H.Corrective tarsometatarsal arthrodesis for malunion after fracture-dislocation in German[J]. Orthopade,2006,35(4):435-442.
[27] Sangeorzan B J,Veith R G,Hansen S T.Salvage of Lisfranc’s tarsometatarsal joint by arthrodesis[J].Foot Ankle,1990,10(4):193-200.
[28] Rosenberg G A, Patterson B M.Tarsometatarsal (Lisfranc’s)fracture-dislocation[J].Am J Orthop (Belle Mead NJ),1995,Suppl:7-16.
[29] Tan Y H,Chin T W,Mitra A K,et al.Tarsometatarsal (Lisfranc’s)injuries: results of open reduction and internal fixation[J].Ann Acad Med Singapore,1995,24(6):816-819.
[30] Buzzard B M,Briggs P J.Surgical management of acute tarsometatarsal fracture dislocation in the adult[J].Clin Orthop Relat Res,1998,35(3):125-133.
[31] Lin S S,Bono C M,Treuting R,et al.Limited intertarsal arthrodesis using bone grafting and pin fixation[J].Foot Ankle Int,2000,21(9):742-748.
[32] Ly T V,Coetzee J C.Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation: a prospective, randomized study[J].J Bone Joint Surg Am,2006,88(3):514-520.
[33] Myerson M S.The diagnosis and treatment of injury to the tarsometatarsal joint complex[J].J Bone Joint Surg Br,1999,81(5):756-763.
[34] Sands A K,Grose A.Lisfranc injuries[J].Injury,2004,35(Suppl 2):71-76.
Clinical Research on Postoperative Lisfranc Injury Traumatic Arthritis
GUO Hong-liang,HAN Ya-jun,Yilihamutuoheti.//Medical Innovation of China,2014,11(24):034-037
Objective:Clinical research on Lisfranc injury traumatic arthritis postoperative.Method:19 cases of Lisfranc injury traumatic arthritis postoperative were selected, 15 men and 4 women, aged 21 to 58 (average, 41)years. The patients all were received Lisfranc fractures underwent open/closed reduction and internal fixation (used screw and wire). Fractures were classified as homolateral (n=7), isolated (n=7), and divergent (n=5). 6 patients had open fractures; 8 patients injured 5 tarsometatarsal joints; and 6 patients had pure ligamentous injury. Outcome was assessed using the Maryland foot score(MFS) and the American Orthopedic Foot and Ankle Society (AOFAS) score. Weight-bearing radiographs were evaluated for non-union, subluxation, malalignment, and post-traumatic arthritis.Result:Patients were followed up for 24 to 40 ((average, 30) months. Patients with anatomic reduction achieved higher mean AOFAS foot score (79.3±4.85 vs 67.5±5.13,P=0.0007) and Maryland foot score (80.4±4.11 vs 69.4±6.07,P=0.0009) than did patients with non-anatomic reduction. Post-traumatic arthritis occurred significantly more often in patients with non-anatomic than anatomic reduction (3/5 vs 1/14,P=0.037). 4 patients developed post-traumatic arthritis, one of whom also developed lateral subluxation after implant removal, 2 patients developed flat foot. 2 patients had severe symptoms that limited function, one of whom underwent an arthrodesis. 2 patients with compound fractures developed superficial infections. 3 patients had broken screws.Conclusion:Lisfranc injury patients treated with anatomical repositioning, curative effect is good, seldom develop arthritis.
Post-traumatic arthritis; Lisfranc injury; Open reduction
10.3969/j.issn.1674-4985.2014.24.011
2014-02-19) (本文编辑:蔡元元)
新疆维吾尔自治区科学技术支疆项目计划(指令性)项目(2013911112)
①新疆医科大学第二附属医院 新疆 乌鲁木齐 830063
伊力哈木·托合提
First-author’s address:The Second Affiliated Hospital of Xinjiang Medical University,Urumqi 830063,China



